Download

1 / 37
420 likes | 541 Views
Easy ECG Interpretation. E. Stanton RN MSN/Ed CEN CCRN CFRN. Conduction system contains pacemaker cells 3 unique characteristics: Automaticity - ability to generate electrical impulses Conductivity - ability to pass impulse to next cell

E N D
Easy ECG Interpretation E. Stanton RN MSN/Ed CEN CCRN CFRN
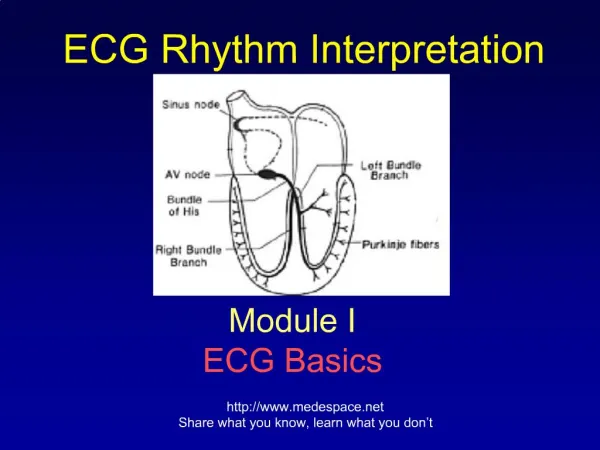
Conduction system contains pacemaker cells 3 unique characteristics: Automaticity- ability to generate electrical impulses Conductivity- ability to pass impulse to next cell Contractility- ability to shorten fibers in the heart when receiving impulses Setting the Pace!
Depolarization-transmission of the impulse through the heart As the electrical impulse moves across the heart cells, polarity (neg or pos charge) of the cells is changed Depolarization is followed by.. Repolarization- Restores the cells to its original charge Depolarization followed by repolarization allows the cells to receive another stimulus KEY TERMS
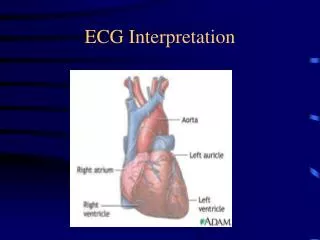
Sinoatrial node (SA node) Pacemaker of the heart Generates impulses between 60- 100/min Sa node fires- spreads impulse through both atria results in atrial contraction Represented by the “P” wave “Feeling Impulsive”
Slows impulse conduction between atria and ventricles Allows time for contracting atria to fill ventricles with blood before lower chambers contract Intrinsic rate 40-60 bpm Represented by the QRS complex The AV Node
Contracting • From AV node impulse travels to: • Bundle of His (right and left) • Purkinje Fibers • As impulse spreads it “informs” the blood filled ventricles to contract and pump blood out
2 built in safety mechanisms if SA node fails- “ Conduction system goes to “plan B” AV node will fire at 40-60 bpm And… if AV node fails- Ventricles generate their own impulse at 20- 40 bpm Back up Systems
ECGis a visible record of heart electrical activity. A stylus traces activity on a continuously moving strip HOW TO READ AN ECG
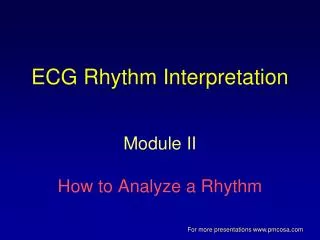
Each beat manifests as 5 major waves: P Q R S T. Each beat begins with a normal shaped P wave Followed by a normal looking QRS (complex) Normal Single Heart Beat
P Wave -first upward deflection- atrial depolarization PR interval- beginning of P wave to onset of QRS- conduction of impulse through atria into AV node QRS complex- 3 deflections: Q- down stroke before the R wave R- 1st upward deflection S- down stroke following R wave ST Segment- begins at the end of the S wave ends at beginning of T wave T wave- represents electrical recovery of the ventricle Making Sense of the Alphabet
Rythym Nation Alphabet Soup
Normal Sinus Rhythm • the conduction starts in the SA node and follows the expected conduction path. Rate is between 60-100bpm.
Heart rate less than 60 bpm Causes- drug toxicity, CAD, intracranial tumors, sleep, electrolyte imbalance, Vomiting and vaso vagal responses (bearing down) Can be a normal finding in athletic people. If asymptomatic no treatment indicated Treatment for symptomatic bradycardia- atropine, pacemaker Sinus Bradycardia
Heart rate 100- 150 bpm Limited time for ventricular filling, less blood pumped into the body Causes- exercise stress fever medications pain anemia heart failure caffeine Tobacco, dehydration Tachycardia Treatment- based on causative factors*
Atrial Dysrhythmias
Atrial Dysrrhythmias • disturbance in the electrical conduction in the atria • Affects the P wave • Causes: • Electrolyte imbalances • Conduction diseases • MI • CHF • stress • drugs
Ectopic impulse not originating in the SA node Often benign, not treated unless symptomatic. Can be a normal occurrence on occasion If the PACs cause symptoms they need evaluation a normal QRS complex a normal T wave repolarization an odd, misshapen P wave PAC
Causes • Ischemia • CHF • Digitalis toxicity • hypokalemia. • Frequent PACs can lead to more serious complications if not treated properly
Erratic electrical activity of the atria atria quiver rather than conduct. Atrial rate of 300-600 bpm Heart rate is regularly irregular Absence of a p wave AV node is bombarded with impulses and randomly transmits the impulses to the ventricles A FIB
Causes of A- Fib • mitral valve disease • CAD • MI • heart failure • cardiomyopathy High risk for clot formation due to blood stasis in the atria-, pt should be anticoagulated
Beta Blockers • block" the action of adrenaline on beta receptors in the cells of heart. • Stronger and slower • slows conduction • makes the AV Node less sensitive to A-Fib impulses Lopressor Tenormin Inderal Toprol Medications
Digoxin-slows down and controls rate by blocking the electrical conduction between the atria and ventricles. Must check levels for toxic/ therapeutic levels Coumadin Anticoagulant, lowers the risk of an unwanted blood clot forming in the heart extremely important to follow the exact dosing prescribed and to have regular blood tests (INR) Medications
Calcium Channel Blockers • prevent or slow the flow of calcium ions into smooth muscle cells • Cardizem • Verapamil • Calan • Isoptin • If no response to medical TX may require cardioversion
Rapid conduction of the AV node Similar to a fib but the p waves are saw tooth in nature Treatment is the same A- Flutter
Ventricular Dysrrhythmia s
Premature Ventricular Contraction- (PVC) Ectopic beat within the ventricles Most common Ectopic beat* Wide, bizarre QRS complex no P waves before the QRS complex Usually followed by a compensatory pause Non life threatening if isolated PVC'S
PVC'S Causes- • electrolyte imbalance • ischemia • Digoxin toxicity • hypoxia • caffeine • anxiety • Treatment-Lidocaine, Amiodarone Oxygen
Ventricular Tachycardia Life threatening arrhythmia requires immediate intervention Occurrence of three or more PVCs. Complete disruption of the electrical activity of the conduction system Ventricular rate may exceed 200 bpm. hypotension, absent peripheral pulses. These beats do not conduct. Eventually become unconscious Ventricle beats so rapidly that it is unable to fill or eject blood. Can lead to ventricular fibrillation I may be in trouble here
Causes- MI electrolyte imbalances (magnesium, calcium, potassium) electrocution Treatment-Procanamide (procan) Lidocaine amiodarone magnesium/calcium (if electrolyte imbalance) defibrillation
Life threatening fatal arrhythmia Disorganized, chaotic, quivering of the ventricles Ventricles are unable to contract- no blood is ejected ECG is a series of jagged unidentifiable waves VENTRICULAR FIBRILLATION Now I know I’m in big trouble
Causes- CAD MI electrolyte imbalance electrocution hypovolemia. Most common cause is CAD* Treatment- Immediate CPRdefibrillation Lidocaine Amiodarone treat electrolyte imbalance
Ventricular fibrillation Time to act quick!
Asystole • Asystole • Straight line • Absence of cardiac activity • This is a full cardiac arrest • Initiate CPR immediately defibrillation and ACLS drugs (Atropine, epinephrine)
Delivery of synchronized electric shock to restore normal cardiac conduction. Shock on R wave** If the shock is delivered during ventricular depolarization it can cause ventricular tachycardia Can be done electively if patient is in a fib, stable and unresponsive to medications cardioversion
defibrillation • Delivery of an unsynchronized high energy electrical shock during an emergent situation. (cardiac arrest) • Patients with recurrent v-tach /v-fib have an AICD placed • AICD -implanted defibrillator usually with a back up pacemaker. detects fatal arrhythmia and delivers a shock to the patient to restore NSR