Download

1 / 42
440 likes | 680 Views
Trends in fungal diseases. Dr David W. Denning FRCP FRCPath Scientific Advisor to the Fungal Research Trust Clinician, Wythenshawe Hospital Head, Antifungal Testing Laboratory Faculty, University of Manchester WWW.aspergillus.man.ac.uk. Trends in fungal diseases.

E N D
Trends in fungal diseases Dr David W. Denning FRCP FRCPath Scientific Advisor to the Fungal Research Trust Clinician, Wythenshawe Hospital Head, Antifungal Testing Laboratory Faculty, University of Manchester WWW.aspergillus.man.ac.uk
Trends in fungal diseases Increasing cases of invasive fungal infections Poor diagnostic tools Replacement of sensitive species by resistant ones Increasing use of prophylaxis and empirical therapy Continuing high frequency of skin infection Increasing awareness of the role of fungi in allergy Increasing drug and hospitalisation costs
Trends in fungal diseases Increasing cases of invasive fungal infections
Increasing rate of candidiasis in the US +600% +300% +300% Martin et al, NEJM 2003;348:1546
Invasive Candida infections in the USA The NEMIS study • 6 Surgical Intensive Care Units in USA • Overall rate 9.82/1000 admissions or 0.98/1000 patient days (range 0.28-1.78) • 48% C. albicans • Mortality of Candida bloodstream infections 41% vs 8% in those without Blumberg HM et al, Clin Infect Dis 2001:33 177-86
Candida bloodstream infections in the UK 2 year prospective study in 6 UK hospitals• 18.7 candidaemias /100,000 FTE’s, or 3 per 100,000 bed days• 45% in ICU • C. albicans in 65% • Majority of isolates susceptible to fluconazole • Outcome improved by removal of catheter Kibbler CC et al, J Hosp Infect 2003;54:18
8 6 4 2 0 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 Prevalence of invasive aspergillosis at autopsy All other Candida spp. Aspergillus spp. In 1992 60% of the IA patients were diagnosed at autopsy and had no treatment Prevalence at Autopsy [%] Groll et al, J Infect 1996;33:23-32.
Changing incidence of fatal invasive mycoses in non-HIV patients in USA Rate per 100,000 population 0.0 0.2 0.4 0.6 0.8 Candidiasis Aspergillosis 1981 1986 1991 1996 McNeil et al, Clin Infect Dis 2001;33:641
Patient group No. (2002) % Candida No Candida % Aspergillus No. Aspergillus AlloBMTx 793 4 32 10 79 Solid organ Tx 2953 5 148 1.9 56 Leukaemia 16269 3 488 6 976 Solid tumour (neutropenic) 28955 3 869 2 579 Advanced cancer 131678 1 1316 1.5 1975 ICU 210130 1 2101 0.2 420 Burns 378 5.6 21 1.9 7 Renal dialysis 24536 0.2 490 0.02 5 AIDS 661 0.2 1 4 26 Total 5466 4120 Predicted numbers of Candida and Aspergillus infections in the UK
Comparative frequencies of other medical conditions in the UK Number New HIV infections (2001) 4,731 Deaths due to hospital acquired infection (estimate) 5,000 New cases of TB (2003) 6,300 Meningitis (2002) 3,000
Invasive fungal infection – current mortality rates Mortality Aspergillosis Pulmonary aspergillosis 50-75% Cerebral aspergillosis 95% Candidiasis Candidaemia 40%
Case fatality rate with amphotericin B Lin et al Clin Infect Dis 2001;32:258
Trends in fungal diseases Increasing cases of invasive fungal infections Poor diagnostic tools
8 6 4 2 0 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 Prevalence of invasive aspergillosis at autopsy All other Candida spp. Aspergillus spp. In 1992, 60% of the patients were undiagnosed and untreated In 1992 60% of the IA patients were diagnosed at autopsy and had no treatment Prevalence at Autopsy [%] Groll et al, J Infect 1996;33:23-32.
Trends in fungal diseases Increasing cases of invasive fungal infections Poor diagnostic tools Replacement of sensitive species by resistant ones
Antifungal susceptibility in Candida spp. Usually susceptible Less susceptible Resistant Fluconazole C. albicans C. tropicalis C. glabrata C. parapsilosis C. krusei All others Amphotericin B C. albicans C. lusitaniae C. krusei C. tropicalis C. glabrata C. parapsilosis Caspofungin C. albicans C. parapsilosis C. tropicalis C. guilliermondii C. glabrata C. lusitaniae C. krusei
Candida glabrata and Candida krusei • Fluconazole intermediate or resistant • Respond poorly to amphotericin B treatment • Increasingly common Candida krusei Candida glabrata
Biofilms and Candida parapsilosis • 2nd most common species in blood, related to catheters and glucose solutions • Causes biofilms which usually require removal of catheters etc, as antifungal drugs are ineffective in eradicating biofilms Infected pacemaker and heart valve, after death
Candida bloodstream infections in European cancer patients Prospective study of candidaemia in European cancer centres• 289 episodes • C. albicans in 70% of cancer and 36% of leukaemia patients • Other species – C. parapsilosis (27) - C. tropicalis (23) - C. glabrata (21) - C. krusei (21) - C. guilliermondii (11) - other Candida spp. (7) Viscoli C et al, Clin Infect Dis 1999;28:1071
A. nidulans – may be amphotericin B resistant Sometimes amphotericin B resistant Low frequency of azole resistance A. terreus – resistant to AmB Aspergillus – 38 species have caused disease Common in the environment www.aspergillus.man.ac.uk
Trends in fungal diseases Increasing cases of invasive fungal infections Poor diagnostic tools Replacement of sensitive species by resistant ones Increasing use of prophylaxis and empirical therapy
Prophylaxis in the surgical intensive care unit • Fluconazole vs. placebo in extremely high risk surgical intensive care patients • Placebo: 16% rate of invasive candidiasis • Fluconazole: 8% rate Pelz et al, Ann Surg 2001;233:542-548,
NEMIS study Antifungal drugs protective (Relative risk 0.3) Blumberg HM et al, Clin Infect Dis 2001:33 177-86
Trends in fungal diseases Increasing cases of invasive fungal infections Poor diagnostic tools Replacement of sensitive species by resistant ones Increasing use of prophylaxis and empirical therapy Continuing high frequency of skin infection
Scalp ringworm in children Increase in reported cases from: 27 in 1980 to 1227 in 2000 Reported carriage rate 12-47% in London primary school children Fuller Br Med J 2003;326:539
Toenail infections Reported frequency 2.8% of adults (1992). More recent European surveys suggest 5-25%, especially in the elderly If 5%, then >2,500,000 cases in the UK 60% treatment (3-6 months) prescribed by GPs without laboratory confirmation 20% failure rate Roberts, Br J Dermatol 1992;126 (Suppl 39):23-7 Pierard, Dermatology 2001;202:220-4.
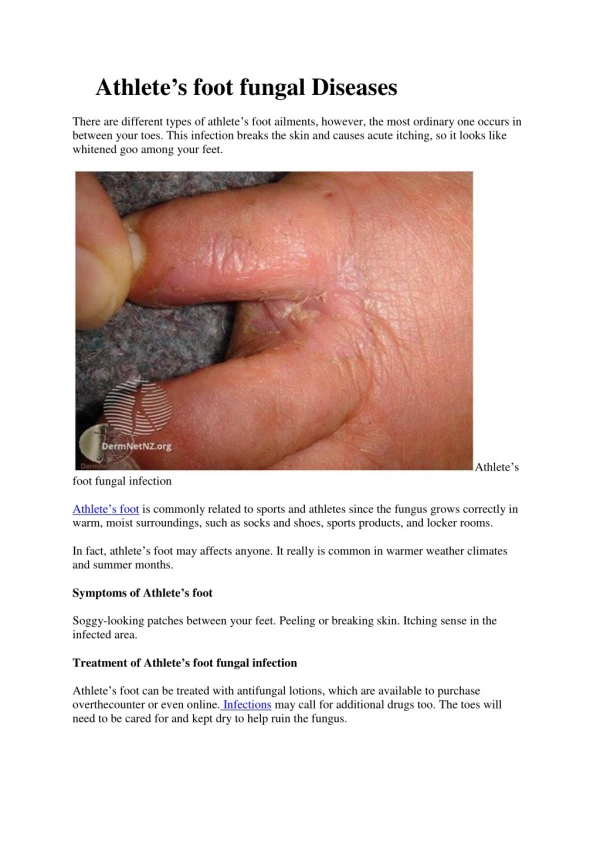
Athlete’s foot and cellulitis Athlete’s foot leads to skin breaks between the toes Bacteria may enter, leading to cellulitis 3% of UK general medical admissions are due to cellulitis
Trends in fungal diseases Increasing cases of invasive fungal infections Poor diagnostic tools Replacement of sensitive species by resistant ones Increasing use of prophylaxis and empirical therapy Continuing high frequency of skin infection Increasing awareness of the role of fungi in allergy
Interaction of Aspergillus with peopleA unique microbial-host interaction Invasive aspergillosis Allergic aspergillosis Frequency of aspergillosis Frequency of aspergillosis Chronic pulmonary Immune dysfunction Immune hyperactivity .
Spore counts and asthma attacks and admission to hospital • All circumstantial evidence • Thunderstorm asthma – linked to Alternaria • Asthma deaths (Chicago) linked to high ambient spores counts and season (summer autumn) when spore counts highest • Asthma hospital admission linked to high ambient spore counts (Derby, New Orleans, Ottawa) • Asthma hospital attendance linked to high spore counts, but not pollen counts (Canada) • Asthma symptoms increased on days of high spore counts (California, Pennsylvania) O'Hollaren, N Engl J Med 1991; 324: 359; Newson, Occup Environ Med 2000; 57: 786-92.
Fungus at home • Environmental data • Mouldy housing associated with worse asthma, with a correlation between asthma severity and degree of dampness in the home and separately with visible mould growth • In Germany bronchial reactivity in children was associated with damp housing • Mouldy and damp school associated with asthma symptoms and emergency room visits • Highest concentration of Aspergillus fumigatus is at home Williamson, Thorax 1997;52:229. Taskinen, Acta Paediatr 1999; 88:1373.
Hospital admission with asthmatic attacks and mould allergy Allergen Asthma, no admission (n=82) Asthma, 2+ admission (n=46) House dust mite 56 % 67 % Grass pollen 46 % 63 % Cat 37 % 59 % Dog 18 % 48 % Any non fungal allergen 70% 74% O’Driscoll et al, BioMed Central, 2004
Hospital admission with asthmatic attacks and mould allergy Allergen Asthma, no admission (n=82) Asthma, 2+ admission (n=46) Aspergillus 7 % 37 % Alternaria 5 % 26 % Cladosporium 1 % 41 % Penicillium 2 % 30 % Candida 10 % 33 % Any fungal allergen 16% 76% O’Driscoll et al, BioMed Central, 2004
Severe asthma and moulds Severe asthma – 235 (21%) of all asthmatics Odds ratio Increasing frequency of fungal skin test positivity in severe asthma Zureik et al, Br Med J 2002;325:411
Asthma severity, house dust mites, cats and moulds * p = 0.05 # p = 0.01 Langley, ATS 2004
Trends in fungal diseases Increasing cases of invasive fungal infections Poor diagnostic tools Replacement of sensitive species by resistant ones Increasing use of prophylaxis and empirical therapy Continuing high frequency of skin infection Increasing awareness of the role of fungi in allergy Increasing drug and hospitalisation costs
Total addressable worldwide market for antifungal drugs Current estimate $5.2 billion Growing 20% annually
Current US antifungal market for injectables (2003) IV Antifungal treatments - $700M Treatments for invasive candidiasis 76% of fungal infections 49% of market dollars Treatments for oesophageal candidiasis 5% of fungal infections 2% of market dollars Treatments for invasive aspergillosis 19% of fungal infections 49% of market dollars
Current drug costs in the UK (per typical course) Indication IV Oral Candida in hospital (fluconazole) £820 Candida in hospital (caspofungin) £4,676 Aspergillus in hospital (AmBisome) £5,538 Aspergillus in hospital (Voriconazole) £1,688 Toenail infections (terbinafine) £536 Vaginal thrush suppression (fluconazole) £850 Chronic pulmonary aspergillosis (voriconazole) £20,506
UK antifungal expenditure GP / community sales 100 Hospital sales 80% increase 20% per year Total sales 80 60 Annual expenditure (£M) 40 20 2003 1999 Department of Health Prescription Cost Analysis, IMS
Indirect costs Additional length of hospital stay (candidaemia) 15-36 days Extra costs of each patient with aspergillosis $62,500 (£35,000) (1999 in US)
Trends in fungal diseases Increasing cases of invasive fungal infections Poor diagnostic tools Replacement of sensitive species by resistant ones Increasing use of prophylaxis and empirical therapy Continuing high frequency of skin infection Increasing awareness of the role of fungi in allergy Increasing drug and hospitalisation costs