Download
1 / 1
10 likes | 264 Views
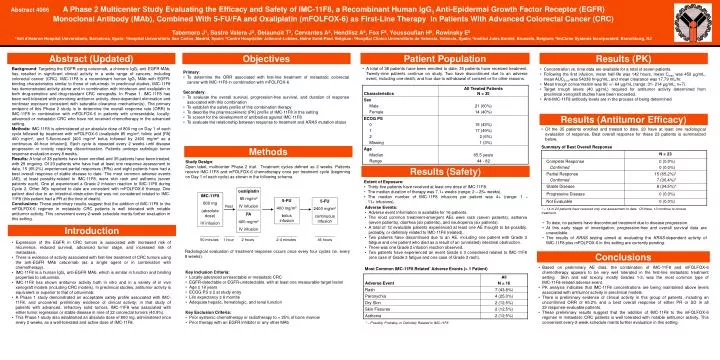
oxaliplatin 85 mg/m 2 IV infusion. IMC-11F8 800 mg (absolute dose) IV infusion. 5-FU 400 mg/m 2 bolus infusion. 5-FU 2400 mg/m 2 continuous infusion. Rest. FA 400 mg/m 2 IV infusion. 1 hour. 2-4 minutes. 46 hours. 50 minutes. 2 hours.

E N D
oxaliplatin 85 mg/m2 IV infusion IMC-11F8 800 mg (absolute dose) IV infusion 5-FU 400 mg/m2 bolus infusion 5-FU 2400 mg/m2 continuous infusion Rest FA 400 mg/m2 IV infusion 1 hour 2-4 minutes 46 hours 50 minutes 2 hours Abstract 4066A Phase 2 Multicenter Study Evaluating the Efficacy and Safety of IMC-11F8, a Recombinant Human IgG1 Anti-Epidermal Growth Factor Receptor (EGFR) Monoclonal Antibody (MAb), Combined With 5-FU/FA and Oxaliplatin (mFOLFOX-6) as First-Line Therapy in Patients With Advanced Colorectal Cancer (CRC) Tabernero J1, Sastre Valera J2, Delaunoit T3, Cervantes A4, Hendlisz A5, Fox F6, Youssoufian H6, Rowinsky E6 1Vall d'Hebron Hospital Universitario, Barcelona, Spain; 2Hospital Universitario San Carlos, Madrid, Spain; 3Centre Hospitalier Jolimont-Lobbes, Haine Saint-Paul, Belgium; 4Hospital Clinico Universitario de Valencia, Valencia, Spain; 5Institut Jules Bordet, Brussels, Belgium; 6ImClone Systems Incorporated, Branchburg, NJ Abstract (Updated) Objectives Patient Population Results (PK) • A total of 38 patients have been enrolled to date; 35 patients have received treatment. Twenty-nine patients continue on study. Two have discontinued due to an adverse event, including one death, and four due to withdrawal of consent or for other reasons. Background: Targeting the EGFR using cetuximab, a chimeric IgG1 anti-EGFR MAb, has resulted in significant clinical activity in a wide range of cancers, including colorectal cancer (CRC). IMC-11F8 is a recombinant human IgG1 MAb with EGFR-binding characteristics similar to those of cetuximab. In preclinical studies, IMC-11F8 has demonstrated activity alone and in combination with irinotecan and oxaliplatin in both drug-sensitive and drug-resistant CRC xenografts. In Phase 1, IMC-11F8 has been well-tolerated with promising antitumor activity, dose-dependent elimination and nonlinear exposure consistent with saturable clearance mechanism(s). The primary endpoint of this Phase 2 study is to determine the overall response rate (ORR) to IMC-11F8 in combination with mFOLFOX-6 in patients with unresectable, locally-advanced or metastatic CRC who have not received chemotherapy in the advanced setting. Methods: IMC-11F8 is administered at an absolute dose of 800 mg on Day 1 of each cycle followed by treatment with mFOLFOX-6 (oxaliplatin 85 mg/m², folinic acid [FA] 400 mg/m², and 5-fluorouracil [400 mg/m² bolus followed by 2400 mg/m² as a continuous 46-hour infusion]). Each cycle is repeated every 2 weeks until disease progression or toxicity requiring discontinuation. Patients undergo radiologic tumor response evaluation every 8 weeks. Results: A total of 38 patients have been enrolled and 35 patients have been treated, with 29 ongoing. Of 23 patients who have had at least one response assessment to date, 15 (65.2%) experienced partial responses (PRs) and eight patients have had a best overall response of stable disease to date. The most common adverse events (AE), at least possibly-related to IMC-11F8, were skin rash and asthenia (seven patients each). One pt experienced a Grade 2 infusion reaction to IMC-11F8 during Cycle 2. Other AEs reported to date are consistent with mFOLFOX-6 therapy. One patient died due to an intestinal obstruction that was not considered related to IMC-11F8 (this patient had a PR at the time of death). Conclusions: These preliminary results suggest that the addition of IMC-11F8 to the mFOLFOX-6 regimen in metastatic CRC patients is well tolerated with notable antitumor activity. This convenient every-2-week schedule merits further evaluation in this setting. • Concentration vs. time data are available for a total of seven patients. • Following the first infusion, mean half-life was 142 hours, mean Cmax was 459 µg/mL, mean AUC0-inf was 54338 hr•µg/mL, and mean clearance was 17.79 mL/hr. • Mean trough concentration was 90 +/- 64 µg/mL (range: 31- 214 µg/mL; n=7). • Target trough levels (40 µg/mL) required for antitumor activity determined from preclinical xenograft studies have been exceeded. • Anti-IMC-11F8 antibody levels are in the process of being determined. • Primary: • To determine the ORR associated with first-line treatment of metastatic colorectal cancer with IMC-11F8 in combination with mFOLFOX-6 • Secondary: • To evaluate the overall survival, progression-free survival, and duration of response associated with this combination • To establish the safety profile of this combination therapy • To describe the pharmacokinetic (PK) profile of IMC-11F8 in this setting • To screen for the development of antibodies against IMC-11F8 • To evaluate the relationship between response to treatment and KRAS mutation status Results (Antitumor Efficacy) • Of the 35 patients enrolled and treated to date, 23 have at least one radiological evaluation of response. Best overall response for these 23 patients is summarized below. Summary of Best Overall Response Methods Study Design: Open label, multicenter Phase 2 trial. Treatment cycles defined as 2 weeks. Patients receive IMC-11F8 and mFOLFOX-6 chemotherapy once per treatment cycle (beginning on Day 1 of each cycle) as shown in the following schema. Results (Safety) • Extent of Exposure: • Thirty-five patients have received at least one dose of IMC-11F8. • The median duration of therapy was 7.1+ weeks (range: 2 – 25+ weeks). • The median number of IMC-11F8 infusions per patient was 4+ (range: 1 – 11+ infusions). • Adverse Events: • Adverse event information is available for 16 patients. • The most common treatment-emergent AEs were rash (seven patients), asthenia (seven patients), diarrhea (six patients), and neutropenia (six patients). • A total of 12 evaluable patients experienced at least one AE thought to be possibly, probably, or definitely related to IMC-11F8 (related). • Two patients have discontinued due to an AE, including one patient with Grade 3 fatigue and one patient who died as a result of an (unrelated) intestinal obstruction. • There was one Grade 2 infusion reaction observed. • Two patients have experienced an event Grade ≥ 3 considered related to IMC-11F8 (one case of Grade 3 fatigue and one case of Grade 3 rash). * – 14 of 23 patients have received only one assessment to date. Of these, 10 continue to receive treatment. • To date, no patients have discontinued treatment due to disease progression. • At this early stage of investigation, progression-free and overall survival data are unavailable. • The results of KRAS testing aimed at evaluating the KRAS-dependent activity of IMC-11F8 plus mFOLFOX-6 in this setting are currently pending. Introduction • Expression of the EGFR in CRC tumors is associated with increased risk of recurrence, reduced survival, advanced tumor stage, and increased risk of metastasis. • There is evidence of activity associated with first-line treatment of CRC tumors using the anti-EGFR MAb cetuximab (as a single agent or in combination with chemotherapy). • IMC-11F8 is a human IgG1 anti-EGFR MAb, which is similar in function and binding properties to cetuximab. • IMC-11F8 has shown antitumor activity both in vitro and in a variety of in vivo xenograft models (including CRC models). In preclinical studies, antitumor activity is equivalent or superior to that of cetuximab. • A Phase 1 study demonstrated an acceptable safety profile associated with IMC-11F8, and uncovered preliminary evidence of clinical activity; in that study of patients with advanced, refractory solid tumors, IMC-11F8 was associated with either tumor regression or stable disease in nine of 22 colorectal tumors (40.9%). • This Phase 1 study also established an absolute dose of 800 mg, administered once every 2 weeks, as a well-tolerated and active dose of IMC-11F8. Radiological evaluation of treatment response occurs once every four cycles (ie, every 8 weeks). Conclusions • Based on preliminary AE data, the combination of IMC-11F8 and mFOLFOX-6 chemotherapy appears to be very well tolerated in the first-line metastatic treatment setting. Skin and nail toxicity, mostly Grades 1-2, was the most common type of IMC-11F8-related adverse event. • PK analysis indicates that IMC-11F8 concentrations are being maintained above levels associated with antitumor activity in preclinical models. • There is preliminary evidence of clinical activity in this group of patients, including an unconfirmed ORR of 65.2% and a best overall response of either PR or SD in all 23 response-evaluable patients. • These preliminary results suggest that the addition of IMC-11F8 to the mFOLFOX-6 regimen in metastatic CRC patients is well tolerated with notable antitumor activity. This convenient every-2-week schedule merits further evaluation in this setting. Most Common IMC-11F8 Related* Adverse Events (> 1 Patient) • Key Inclusion Criteria: • Locally-advanced unresectable or metastatic CRC • EGFR-detectable or EGFR-undetectable, with at least one measurable target lesion • Age ≥ 18 years • ECOG PS ≤ 2 at study entry • Life expectancy ≥ 6 months • Adequate hepatic, hematologic, and renal function • Key Exclusion Criteria: • Prior systemic chemotherapy or radiotherapy to > 25% of bone marrow • Prior therapy with an EGFR inhibitor or any other MAb * – Possibly, Probably, or Definitely Related to IMC-11F8