Download
1 / 1

E N D
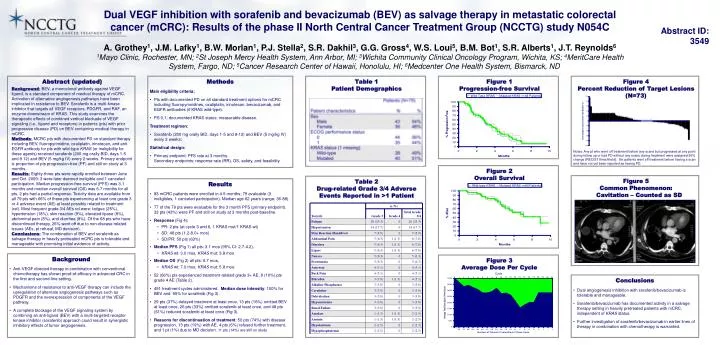
Abstract (updated) Background:BEV, a monoclonal antibody against VEGF ligand, is a standard component of medical therapy of mCRC. Activation of alternative angiogenesis pathways have been implicated in resistance to BEV. Sorafenib is a multi-kinase inhibitor that targets all VEGF receptors, PDGFR, and RAF, an enzyme downstream of KRAS. This study examines the therapeutic effects of combined vertical blockade of VEGF signaling (i.e., ligand and receptors) in patients (pts) with prior progressive disease (PD) on BEV-containing medical therapy in mCRC. Methods:MCRC pts with documented PD on standard therapy including BEV, fluoropyrimidine, oxaliplatin, irinotecan, and anti-EGFR antibody for pts with wild-type KRAS (or ineligibility for these agents) received sorafenib (200 mg orally BID, days 1-5 and 8 12) and BEV (5 mg/kg IV) every 2 weeks. Primary endpoint is proportion of pts progression-free (PF) and still on study at 3 months. Results:Eighty-three pts were rapidly enrolled between June and Oct. 2009; 3 were later deemed ineligible and 1 canceled participation. Median progression-free survival (PFS) was 3.1 months and median overall survival (OS) was 6.7 months for all pts. 2 pts had a partial response. Toxicity data are available from all 79 pts with 66% of these pts experiencing at least one grade 3 or 4 adverse event (AE) at least possibly related to treatment (rel). Most frequent grade 3/4 AEs rel were: fatigue (25%), hypertension (18%), skin reaction (9%), elevated lipase (8%), abdominal pain (8%), and diarrhea (8%). Of the 68 pts who have discontinued therapy, 26% went off due to non-disease related issues (AEs, pt refusal, MD decision). Conclusions:The combination of BEV and sorafenib as salvage therapy in heavily pretreated mCRC pts is tolerable and manageable with promising initial evidence of activity. • Methods • Main eligibility criteria: • Pts with documented PD on all standard treatment options for mCRC including fluoropyrimidines, oxaliplatin, irinotecan, bevacizumab, and EGFR antibodies (if KRAS wild-type). • PS 0,1; documented KRAS status; measurable disease. • Treatment regimen: • Sorafenib (200 mg orally BID, days 1-5 and 8-12) and BEV (5 mg/kg IV) every 2 weeks; • Statistical design: • Primary endpoint: PFS rate at 3 months.Secondary endpoints: response rate (RR), OS, safety, and feasibility. Table 1 Patient Demographics Figure 3 Average Dose Per Cycle Cycle Figure 4 Percent Reduction of Target Lesions (N=73) • Results • 83 mCRC patients were enrolled in 4.5 months; 79 evaluable (3 ineligibles, 1 canceled participation). Median age 62 years (range: 36-88). • 77 of the 79 pts were evaluable for the 3 month PFS (primary endpoint). 33 pts (43%) were PF and still on study at 3 months post-baseline. • Response (Fig 4): • PR: 2 pts (at cycle 3 and 6, 1 KRAS mut/1 KRAS wt) • SD: 48 pts (1.2-8.0+ mos) • SD/PR: 50 pts (63%) • Median PFS (Fig 1) all pts: 3.1 mos (95% CI: 2.7-4.2), • KRAS wt: 3.0 mos, KRAS mut: 3.8 mos • Median OS (Fig 2) all pts: 6.7 mos, • KRAS wt: 7.0 mos; KRAS mut: 5.8 mos. • 52 (66%) pts experienced treatment-related grade 3+ AE; 8 (10%) pts grade 4 AE (Table 2). • 491 treatment cycles administered. Median dose intensity: 100% for BEV and 95% for sorafenib (Fig 3). • 29 pts (37%) delayed treatment at least once, 13 pts (16%) omitted BEV at least once, 26 pts (33%) omitted sorafenib at least once, and 48 pts (61%) reduced sorafenib at least once (Fig 3). • Reasons for discontinuation of treatment: 50 pts (74%) with disease progression, 13 pts (19%) with AE, 4 pts (6%) refused further treatment, and 1 pt (1%) due to MD decision. 11 pts (14%) are still on study Notes: Any pt who went off treatment before any scans but progressed at any point during follow up or had PD without any scans during treatment were assigned 30% change (RECIST threshhold). Six patients went off treatment before having a scan and have not yet been reported as having PD. • Background • Anti-VEGF directed therapy in combination with conventional chemotherapy has shown proof-of-efficacy in advanced CRC in the first and second-line setting. • Mechanisms of resistance to anti-VEGF therapy can include the upregulation of alternate angiogenesis pathways such as PDGFR and the overexpression of components of the VEGF pathway. • A complete blockage of the VEGF signaling system by combining an anti-ligand (BEV) with a multi-targeted receptor kinase inhibitor (sorafenib) approach could result in synergistic inhibitory effects of tumor angiogenesis. Dual VEGF inhibition with sorafenib and bevacizumab (BEV) as salvage therapy in metastatic colorectal cancer (mCRC): Results of the phase II North Central Cancer Treatment Group (NCCTG) study N054C Abstract ID: 3549 • Grothey1, J.M. Lafky1, B.W. Morlan1, P.J. Stella2, S.R. Dakhil3, G.G. Gross4, W.S. Loui5, B.M. Bot1, S.R. Alberts1, J.T. Reynolds6 • 1Mayo Clinic, Rochester, MN; 2St Joseph Mercy Health System, Ann Arbor, MI; 3Wichita Community Clinical Oncology Program, Wichita, KS; 4MeritCare Health System, Fargo, ND; 5Cancer Research Center of Hawaii, Honolulu, HI; 6Medcenter One Health System, Bismarck, ND Figure 1 Progression-free Survival Figure 2 Overall Survival Figure 5 Common Phenomenon: Cavitation – Counted as SD Table 2 Drug-related Grade 3/4 Adverse Events Reported in >1 Patient • Conclusions • Dual angiogenesis inhibition with sorafenib/bevacizumab is tolerable and manageable. • Sorafenib/bevacizumab has documented activity in a salvage therapy setting in heavily pretreated patients with mCRC, independent of KRAS status. • Further investigation of sorafenib/bevacizumab in earlier lines of therapy in combination with chemotherapy is warranted.