Download
1 / 72
730 likes | 761 Views
Dive into the anatomy of the knee, learn about ligaments, muscles, and preventing injuries. Detailed information on ACL, PCL, MCL, LCL, and more. Discover ways to strengthen and rehabilitate the knee joint effectively.

E N D
Anatomy and Injuries of the Knee Adapted from Connie Rauser Sabino Sports Medicine
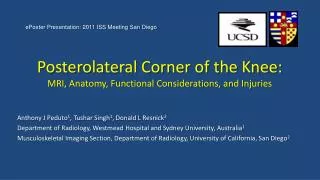
Bones • Femur • Medial/lateral femoral condyles articulate w/ tibia • Tibia • Tibial plateau is flat-articulates w/ femoral condyles • Fibula • Articulates w/ tibia • Patella • Sesamoid bone protects anterior joint • Enclosed in quadriceps/patellar tendon Anatomy-Bones
Joints • Tibiofemoral • Hinge joint with synovial lining • diarthrodial • Patellofemoral • Superior Tibiofibular Anatomy-Joints
Meniscus • Medial and lateral • Fibrocartilaginous disks • Thicker on outside than inside (poor blood supply) • Lie on top of tibial plateau • Increase stability • Make condyles fit better • Shock absorbers Anatomy-Meniscus
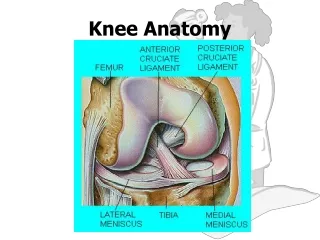
ACL-anterior cruciate ligament • Runs from anterior tibia to posterior femur • Prevents anterior displacement of tibia on fixed femur • Prevents femur from moving posterior during weight bearing • Stabilizes tibia against excessive internal rotation Anatomy-Ligaments
PCL-posterior cruciate ligament • Runs from posterior tibia to anterior femur • Prevents posterior translation of tibia on fixed femur • Prevents femur from moving anterior during weight bearing • Both ACL and PCL “cross” or wrap around each other—taut when in extension and looser when in flexion Ligaments
MCL-medial collateral ligament • Attaches on the medial femoral epicondyle & anteromedial tibia • Thickened portion of joint capsule • Two parts-superficial and deep • Deep portion attaches to medial meniscus • Stabilizes against valgus stress applied to lateral aspect of joint capsule Ligaments
LCL-lateral collateral ligament • Attaches to lateral femoral epicondyle and head of fibula • Stabilizes against varus stress when force is applied to medial aspect of joint • Both the MCL and LCL are tightest during full extension of knee and relaxed during flexion Ligaments
Quadriceps • Rectus femoris, vastus lateralis, vastus medialis, vastus intermedius • Knee extension, hip flexion • Hamstrings • Biceps femoris, semimembranosus, semitendinosus • Knee flexion, hip extension Muscles
Gracilis • Knee flexion, hip adduction • Sartorius • Knee flexion, hip flexion, hip external rotation • Popliteus • Knee flexion • Gastrocnemius • Knee flexion Muscles
Plantaris • Knee flexion • Pes anserine • Goose’s foot • Knee flexion, some internal rotation • Gracilis, sartorius, semitendinosus • Iliotibial Band • Thick band on lateral aspect of thigh • Attaches at Gerdy’s tubercle on the lateral aspect of tibia Muscles
Conditioning • Strength, flexibility, cardiovascular and muscular endurance • Hamstring strength 60% of quad strength • Rehabilitation • Strengthen all muscles around knee joint • Shoes • proper type for surface • Length of cleats • Turf vs grass Preventing knee injuries
Knee braces • Functional vs. prophylactic • Functional—used to provide support to an unstable knee • Usually custom fitted to some degree • Uses hinges and supports to control excessive rotational stress and tibial translation • Prophylactic-worn on lateral aspect knee to protect MCL. • Usefulness questioned—does it cause more injuries? Preventing knee injuries
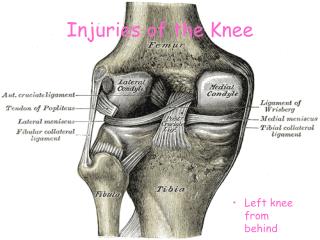
MOI: • fixed foot and external rotation of femur • knee in valgus position • hyperextension • S/S: • “pop”, • knee gives out • instability of knee joint • swelling within knee joint—hemarthrosis • intense pain initially but still able to walk • “+” Lachman’s test • “+” anterior drawer test ACL rupture
Hyperextension MOI
The ACL intact The ACL torn Inside the knee joint
Tx: RICE, knee immobilizer, crutches, Physician referral • Requires surgical reconstruction • Timing of surgery decided by athlete, parents, doctor • Grafts used are patellar tendon, hamstring tendon, cadaver graft, allograft • 3-5 weeks in brace, 6-9 months return to activity ACL Rupture
Knee post-ACL tear • Test for Swelling • Ballotable Patella Test ACL Rupture
Lachman’s test Stress tests
Modified Lachman’s Stress tests
Anterior Drawer test Stress tests
MOI: • hyperflexion • falling on bent knee with foot plantar flexed • Hit on fixed anterior tibia • S/S: • “pop” at the back of knee • Pt. Tender and swelling in popliteal fossa • + posterior sag test,+ posterior drawer test PCL Rupture
Tx: • RICE • Immobilization • Crutches • Physician referral • 6-8 weeks rest/rehab • If surgery is elected, 6 weeks immobilization PCL rupture
Posterior sag Stress tests
Sunrise or posterior sag Stress tests
MOI: • Blow to the lateral side of knee (valgus stress) • External rotation of tibia MCL Sprain
2nd degree?? MCL sprain
S/S: • 1st degree • Pt. Tender over MCL, stable but pain with valgus stress, mild joint effusion, mild joint stiffness, full ROM • 2nd degree • Partial tearing-superficial portion, Pt. Tender over MCL, some instability with valgus stress but solid endpoint, moderate joint effusion, joint stiffness, limited ROM, unable to fully extend knee joint MCL sprain
S/S: • 3rd degree • Complete tear—superficial and deep portions • Pt. Tender over MCL • Moderate to severe effusion • Severe pain • Loss of motion due to pain, effusion, muscle guarding • “+” valgus stress in 0 and 30 degrees, no endpoint MCL Sprain
Valgus stress test @ 0 Valgus stress @ 30 Stress tests for MCL
Tx: • RICE • Crutches • Knee immobilizer/brace • 1st degree 1-2 weeks • 2nd degree 2-4 weeks • 3rd degree 4-6 weeks • Physician referral for 2nd degree or greater MCL Sprain
The terrible triad or unhappy triad • Torn ACL • Torn MCL • Torn Medial meniscus Complications
MOI: • Varus force to medial aspect of knee • internal rotation of tibia • S/S: • Pt. Tender over LCL, • pain, • swelling, • loss of motion, • “+” varus stress at 30 degrees—solid endpoint with 1st degree, less stability but solid endpoint with 2nd degree, no endpoint with 3rd degree • if “+” varus stress at 0 degrees flexion suspect ACL or PCL injury as well LCL sprain
Tx: • RICE • Crutches • Knee immobilizer • Physician referral with 2nd or 3rd degree LCL sprain
Medial: more often torn than later due to attachment to MCL • Lateral: doesn’t attach to joint capsule making it more mobile, less prone to injury • MOI: • Weight bearing with rotational force while extending or flexing the knee Meniscus tear
S/S: • Effusion w/in 48-72 hours • Pt. Tender over joint line • Loss of motion • “locking” • Giving out • Pain with deep knee flexion--squatting Meniscus tear
Types of meniscus tears Meniscus tear
McMurray Test • Positive Sign: Pain and/or clicking Meniscus Tears Special Test
Tx: • RICE • Crutches if necessary • Physician referral • If knee is “locked” by displaced meniscus, go to ER • Arthroscopic surgery to fix Meniscus tears
Dislocation • Subluxation • Fracture • Chondromalacia • Patellar tendonitis Injuries to the Patella
MOI: • Foot planted, deceleration, and cutting in opposite direction from the weight bearing foot • Thigh rotates internally while leg rotates externally • Strong forceful contraction of quads (vastus lateralis) Patella Dislocation
S/S: loss of motion/function at the knee • Pain • Swelling • Deformity • Pt. Tender over medial aspect of knee joint Dislocation
Tx: • immobilize in position you find it • Ice • ER visit • After reduction, immobilize in extension about 4 weeks—use crutches • Strengthen muscles of knee, thigh and hip Dislocation