Download
1 / 82
910 likes | 2.41k Views
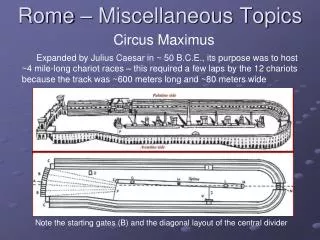
Miscellaneous Nose Topics. Dr. Vishal Sharma. Contents. 1. C.S.F. rhinorrhoea 2. Nasal foreign body 3. Rhinolith 4. Nasal myiasis 5. Choanal atresia. C.S.F. Rhinorrhoea. Introduction. Leakage of cerebrospinal fluid from nose

E N D
Miscellaneous Nose Topics Dr. Vishal Sharma
Contents 1. C.S.F. rhinorrhoea 2. Nasal foreign body 3. Rhinolith 4. Nasal myiasis 5. Choanal atresia
Introduction • Leakage of cerebrospinal fluid from nose • Denotes presence of fistulous communication b/w sub-arachnoid space & nasal cavity • Paradoxical CSF rhinorrhoea:leak of CSF from nose but defect present in mastoid or middle ear roof. CSF enters nasal cavity via Eustachian tube.
Traumatic 1. Accidental (80%):seen in 2% of head injuries 2. Surgical (20%) Endoscopic sinus surgery Surgery for meningocele Trans sphenoidal hypophysectomy Acoustic neuroma surgery
Non-traumatic 1. Normal intracranial pressure (55%) Congenital anomaly Focal atrophy Cough/ strain Osteitis / osteomyelitis Idiopathic 2. High intracranial pressure (45%) Tumor (85%) Hydrocephalus (15%)
Pathways for CSF rhinorrhoea 1. From anterior cranial fossa via: a. Frontal sinus b. Sphenoid sinus c. Ethmoid sinus / Cribriform plate 2. From middle cranial fossa via: a. Sphenoid sinus b. Mastoid cells / middle ear → Eustachian tube 3. From posterior cranial fossa via: a. Sphenoid sinus b. Mastoid cells / middle ear → Eustachian tube
Symptoms 1. Unilateral watery nasal discharge: can’t be sniffed back, sweet taste, increases on bending down & straining 2. H/o head injury, surgery of nose or skull base 3. Headache relieved on reclining or straining: low CSF pressure relieved by rhinorrhoea: high CSF pressure 4. Recurrent meningitis: suspect CSF leak
Signs • Reservoir Sign / Tea Pot Sign: Bending forward produces watery nasal discharge • Halo Sign / Target Sign / Double Ring Sign: CSF mixed with blood produces peripheral CSF halo around central blood on filter paper / pillow cover • Handkerchief sign: Nasal discharge causes stiffening of hanky (due to presence of mucin), but not CSF
Investigations • Nasal discharge biochemistry • Glucose levels (> 30 mg % is CSF) • Beta-2 Transferrin assay positive • CT / MRI head & brain with contrast • Localize site of CSF leak • R/O Tumor • CT Cisternography with Metrizamide/ Ionohexol • Intra-thecal Fluorescein dye Injection + DNE under blue light:fluorescent yellow colored CSF
Intra-thecal Fluorescin Plain DNE Blue light Endoscopy
Conservative management Indications: 1. Immediate post-traumatic leak (within 48 hours) 2. Small post-operative leaks 3. Poor risk patients for surgery
Conservative Treatment • Bed rest in head up position (300) • Avoid coughing, sneezing, nose blowing, straining • Anti-tussive: for dry persistent cough • Laxative: for constipation • Medications: Acetazolamide, Furosemide • Repeated removal of CSF via repeat lumbar taps or indwelling lumbar sub-arachnoid drain • Prophylactic antibiotics to prevent meningitis
Indications for Surgical Rx 1. Non-traumatic CSF rhinorrhoea 2. Failed conservative management for 2 weeks 3. Delayed post-traumatic CSF leak (> 48 hours after trauma) 4. Massive post-operative leaks & recurrent leaks 5. Associated facial fractures 6. Indication for intra cranial exploration: a. Large skull base defect with brain herniation. b. Foreign body penetrating brain 7. Meningitis / pneumocele refractory to conservative Rx by 1 wk
Surgical Approaches Extracranial (endoscopic) Precisely located leak Single, small leak (< 1 cm) Intracranial (preferably intradural) Non-identifiable leaks Large leak (> 1cm) Multiple leaks
4-layer endoscopic repair 1. Bone graft: put intra-cranially as underlay 2. Temporalis fascia / perichondrium: as onlay 3.Fat: over fascia / perichondrium 4. Gel foam / Merocel: over fat
Types of nasal foreign body Inanimate • Vegetable: Pea, maize, gram, bean, nut • Non vegetable: Paper, cotton wool, pencil, eraser, chalk • Mineral: Part of metal / plastic toy, washer, pebble, nail, metal screw, button, sponge, disc battery Animate Maggot, leech, insect
Etiology • Self insertion • Into anterior nares • Accidental insertion • Into posterior nares by vomiting, coughing • Penetrating wounds • Nasal surgery: gauze pack left behind • Palatal perforation
Pathophysiology Neglected FB nose will lead to: • Stasis of secretions & infection • Pressure effects, mucosal damage • Ulceration & granulation formation • Calcification of inspissated mucosa • Rhinolith formation • Leaking disc battery may cause necrosis & septal perforation within hours
Symptoms Inanimate FB Nasal obstruction Purulent or blood-stained nasal discharge Epistaxis Hyposmia Animate FB Sero-sanguinous / foul smelling discharge Formication Marked swelling of nose, cheek, face Fever
Diagnosis • U/L nasal obstruction with blood-stained or foul smelling discharge in children = foreign body until proven otherwise • Foreign body may be seen on anterior rhinoscopy • Foreign body may be hidden behind granulations: felt on probing • X-ray PNS lateral view: show radio-opaque FB • Nasal endoscopy: show radiolucent FB
Treatment • Curved FB hook or Eustachian catheter passed beyond foreign body & FB gently pulled forward • General anesthesia needed for uncooperative pt, impacted or deep foreign body, troublesome bleeding • Leech removed after putting pinch of salt or hypertonic saline or few drops of oxalic acid on their body. • Maggots removed (after putting turpentine oil soaked ribbon gauze pack in nasal cavity) with Tilley forceps
Etiology • Neglected foreign body nose buried in granulations or inspissated nasal secretions or blood clot → forms nucleus (nidus) around which coating of Ca & Mg salts (PO4 + CO3) occurs→ rhinolith formation • Gradually it grows into large, irregular mass filling nasal cavity → pressure necrosis of septum & or lateral nasal wall
Clinical Features • More common in adults • U/L nose block & foul-smelling, blood-stained nasal discharge • Epistaxis & neuralgia due to mucosal ulceration • O/E brown or greyish irregular mass, feels stony hard on probing, brittle & may break off while probing, may be surrounded by granulations
Treatment • Majority removed endoscopically with local anesthesia • Removed under general anesthesia if painful • May be necessary to break & then remove piecemeal • Large rhinolith may require lateral rhinotomy