Download
1 / 31
330 likes | 669 Views
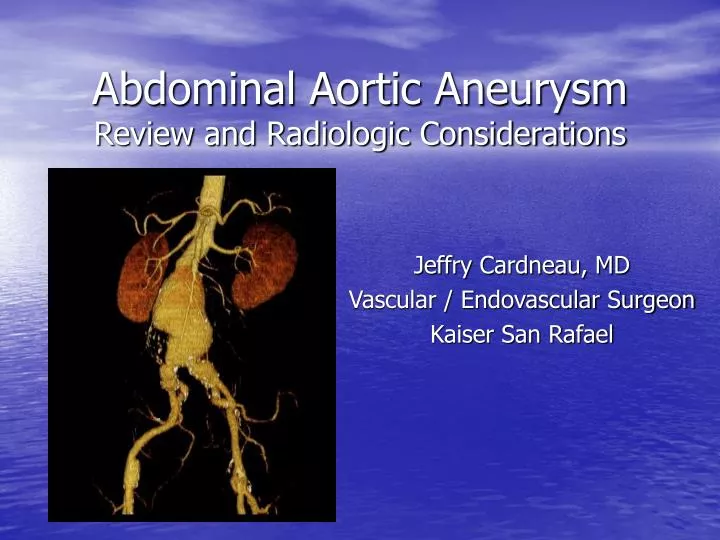
Abdominal Aortic Aneurysm Review and Radiologic Considerations. Jeffry Cardneau, MD Vascular / Endovascular Surgeon Kaiser San Rafael. Objectives. Review History of aneurysm repair Pathophysiology Treatment options and benefits Discuss Endovascular repair Radiologic considerations.

E N D
Abdominal Aortic AneurysmReview and Radiologic Considerations Jeffry Cardneau, MD Vascular / Endovascular Surgeon Kaiser San Rafael
Objectives Review History of aneurysm repair Pathophysiology Treatment options and benefits Discuss Endovascular repair Radiologic considerations
Abdominal Aortic Aneurysm (AAA) First described by Vesalius in 16th century although, other types of aneurysms described in Ebers Papyrus (Egypt, 2000 B.C.) Most common type of true aneurysm 200,000 new cases diagnosed each year 40,000 elective AAA repairs in U.S. annually AAA rupture is 14th leading cause of death in U.S. 15,000 deaths annually from rupture operative mortality for ruptured AAA has not changed in last 20 years prevalence 7.5 % of men older than 65 1.3 % of women older than 65
Aortic Aneurysms Types Thoracic (19%) Thoracoabdominal (2%) Abdominal (AAA) (78%) Infrarenal (95% of all AAA) Juxtarenal Pararenal False aneurysms (pseudoaneurysms) Traumatic anastomotic
AAA Remains an Important Problem 4-8% men have AAA Higher in smokers and pts with CAD (14%) Mortality from ruptured AAA is 80-90% >50% mortality in those who make it to OR
Risk Factors for Detecting a AAA Risk FactorOdds Ratio Smoking history 5.6 Family history of AAA 2.0 Older age (per 7 years interval) 1.7 CAD 1.6 High cholesterol 1.5 COPD 1.3 Height (per 7 cm interval) 1.2 DVT history 0.7 Diabetes 0.6 Black race 0.5 Female gender 0.2 From Lederle FA, et al. Ann Intern Med. 1997;126(6): 441
Abdominal Aortic Aneurysm (AAA) Detection physical exam X rays, CT scans, ultrasounds often done for other reasons and found incidentally most common screening of patients at risk Ultrasound symptoms
Abdominal Aortic Aneurysm (AAA) screening Medicare AAA screening benefit Screening Abdominal Aortic Aneurysms Very Efficiently (SAAAVE) law effective Jan 1, 2007 provided by lobbying from Society of Vascular Surgery part of “Welcome to Medicare physical” for at risk patient men who have smoked sometime in lifetime men and women with family history screening expected to save thousands of lives
Evolution of AAA Repair Focus of early interventions was ligation or banding Results usually poor due to failure to totally exclude the AAA from proximal or distal flow, collateral flow into sac, or erosion of ligatures Matas’ first successful ligation of the human aorta, 1923
Modern Aortic Surgery Homograft insertion an early breakthrough but degeneration soon recognized problems of procurement and availability prosthetic arterial substitutes the true leap forward Dubost’s Operation, 1951
Modern Aortic Surgery • 1947-1948 surgical resident - 1 year research fellowship. • Chance observation that an errant silk suture bridging a dog’s ventricular cavity was coated with a glistening film of what appeared to be endocardium. Speculated that “a piece of cloth might react in a similar way.” • First graft fabricated on his wife’s sewing machine from a silk handkerchief functioned one hour. Arthur Voorhees, MD (1921-1992)
Modern Aortic Surgery • Voorhees’s subsequent work with Blakemore during his residency utilized Vinyon-N, a cloth for spinnaker sails • Original report in 1952 • First human implant in 1953 for ruptured AAA, no homograft available • Forerunner of Dacron fabric graft Vinyon-N Prosthesis 8-year Explant
Results of Open AAA Repair BUT... Effective and Durable • 5-10% mortality in population-based studies • 15-30% significant morbidity; substantially higher in elderly patients with co-morbidity • Recovery 2-3 months • High risk patients often denied repair
Abdominal Aortic Aneurysm (AAA) What size to treat? Traditional threshold was about 5 cm Any advantage to treating earlier (smaller AAA)?
Rupture Risk Low RiskAverage RiskHigh Risk Diameter <5 cm 5-6 cm >6cm Expansion <0.3 cm/year 0.3-0.6 cm/year >0.6 cm/year Smoking/COPD None, mild Moderate Severe/steroids Family history No relatives One relative Numerous relatives Hypertension Normal blood Controlled Poorly controlled pressure Gender Male Female Shape Fusiform Saccular Very eccentric Wall stress Low (35N/cm2) Med(40N/cm2) High (45N/cm2)
Abdominal Aortic Aneurysm (AAA) almost uniformly fatal if AAA ruptures BUT, most AAA never rupture size predicts rupture size (cm)annual rupture risk (%) 4 year rupture < 3 0 0 3 – 3.9 0.4 1.6 4 – 4.9 1.1 4.4 5 – 5.9 3.3 13.2 6 – 6.9 9.4 37.6 7 – 7.9 24 96
Abdominal Aortic Aneurysm (AAA) UK Small Aneurysm Trial Lancet 1998;352:1649-1655. NEJM 2002;346:1445-1452. 1090 patients (age 60 – 79) Aneurysms 4.0 – 5.5 cm Two groups Early elective surgery Observation / surveillance with ultrasound Average follow-up: 8 years Mean duration of survival Early surgery 6.7 years Surveillance 6.5 years
Abdominal Aortic Aneurysm (AAA) ADAM (Aneurysm Detection And Management) NEJM 2002;346(10):1437-1444 1136 patients (ages 50 – 79) Aneurysms 4.0 – 5.5 cm open repair surveillance mean duration of follow-up: 4.9 years operative mortality 2.7 % rate of aneurysm rupture: 0.6 % per year no difference in groups overall survival deaths related to aneurysm
repair methods Open with dacron graft Since 1953 Endovascular repair (EVAR) First done in 1991 by Parodi et al. Abdominal Aortic Aneurysm (AAA)
- Trade Off - ENDOVASCULAR VS. OPEN REPAIR Con Pro Less secure repair Possibility of rupture Chance of device failure Re-interventions Surveillance Cost Risk Procedure time Blood loss ICU LOS Recovery
Preoperative statin therapy in AAAJ Vasc Surg. June 2010;51:1390-6 Reviewed 401 patients to examine perioperative results with statins OPEN REPAIR (228)EVAR (173) statin no statin statin no statin Death (%) 0.0 5.9 0.0 3.6 MI (%) 0.0 3.7 1.1 1.1 Renal failure (%) 0.0 3.7 1.2 2.3 Any comp. (%) 4.4 14.7 4.4 4.8 LOS (days) 8.2 9.1 2.3 2.8 Total cost ($) 18647 22440 33237 36442
EVAR-1 trialLancet 2004; 364: 843-848.Lancet 2005; 365: 2179-2186.
EVAR-1 trialLancet 2004; 364: 843-848.Lancet 2005; 365: 2179-2186. • 1082 patients enrolled 1999 – 2004 • 37 hospitals across UK • all patients > 60 years old • aneurysms > 5.5 cm in diameter • All patients considered “fit” for open or endovascular repair • No financial support from pharmaceutical or device companies
EVAR-1 trialLancet 2004; 364: 843-848.Lancet 2005; 365: 2179-2186. • RESULTS • openendoP value • mean hospital stay (days) 12 7 <.0001 • 30 day mortality 4.6 % 1.6 % .011 • 30 day secondary interventions5.8 % 9.8 % .025 • 4 year aneurysm mortality 7 % 4 % .04 • 4 year cumulative mortality 29 % 26 % .46 • 4 year complication rate 9 % 41 % <.0001 • 4 year reintervention rate 6 % 20 % <.0001 • HRQL (SF36) No difference after 3 months • CONCLUSION
EVAR-1 trialNEJM 2010;362(20):1863-1871. • up to 10 years of followup, with at least 5 years followup • openendoP value • aneurysm related deaths • <6 months (/100 pt-yrs) 10.0 4.6 .03 • >4 years (/100 pt-yrs) 0.2 0.8 • graft related complications • <6 months (/100 pt-yrs) 15.6 48.7 <.001 • >4 years (/100 pt-yrs) 1.4 5.1 <.001 • reinterventions • <6 months (/100 pt-yrs) 13.8 22.9 .007 • >4 years (/100 pt-yrs) 0.8 2.4 .003 • 8 year costs • aneurysm procedures $18,586 $23,153 • does NOT include CTs
Kaplan-Meier Estimates for Total Survival and Aneurysm-Related Survival during 8 Years of Follow-up The United Kingdom EVAR Trial Investigators. N Engl J Med 2010;362:1863-1871
Kaplan-Meier Estimates for the Time to the First Graft-Related Reintervention during 8 Years of Follow-up The United Kingdom EVAR Trial Investigators. N Engl J Med 2010;362:1863-1871
Kaplan-Meier Estimates for the Time to the First Graft-Related Complication during 8 Years of Follow-up The United Kingdom EVAR Trial Investigators. N Engl J Med 2010;362:1863-1871
Operative Mortalityopen vs endo J Vasc Surg 2006;43:446-452