Download
1 / 52
550 likes | 895 Views
Abdominal Aortic Aneurysm Update 2009. Paul Skudder MD FACS. Learning Objectives. Understand the epidemiology and pathogenesis of Abdominal Aortic Aneurysms Be familiar with appropriate diagnostic measures Recognize indications for referral and repair of AAA

E N D
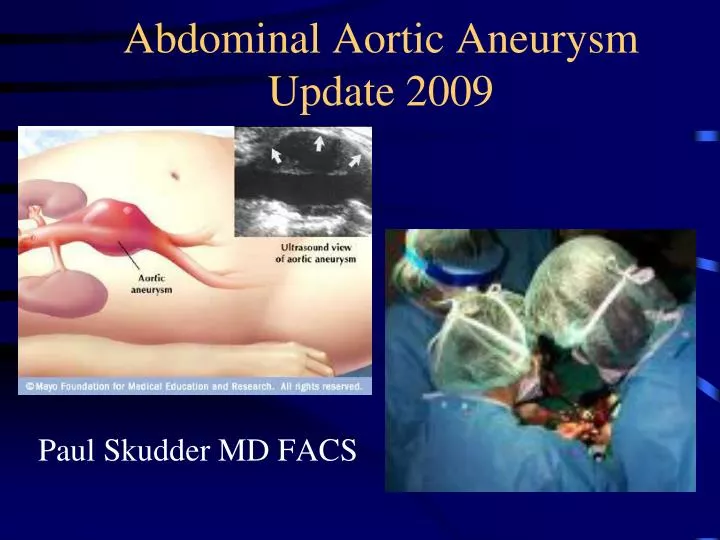
Abdominal Aortic Aneurysm Update 2009 Paul Skudder MD FACS
Learning Objectives • Understand the epidemiology and pathogenesis of Abdominal Aortic Aneurysms • Be familiar with appropriate diagnostic measures • Recognize indications for referral and repair of AAA • Be familiar with available surgical options • Understand role of screening for AAA
Case presentation • 72 year old obese man comes to the ER • Followed annually by primary care • History of BP, smoking and COPD • Sudden onset severe flank and back pain, severe hypotension and hypovolemic shock
Case presentation (2) • CT shows a ruptured 8 cm AAA • Vascular consultation • To OR: Aorta aneurysm repaired at emergency surgery
Case presentation (3) • Patient survives procedure • ICU on ventilator • Passes bloody stool • Emergency endoscopy
Case presentation (4) • Endoscopy shows frank necrosis of the sigmoid colon • Back to surgery • General surgery removes sigmoid colon, leaves patient with colostomy
Case presentation (5) • Patient remains septic in ICU • On ventilator • Profound oliguria and rapidly progressive azotemia • Renal consult
Case presentation (6) • Acute renal failure • Back to surgery • Vascular places a dialysis permcath • Later has AVF surgery for permanent dialysis
Case presentation (7) • Remains on ventilator in ICU • VAP with MRSA • 3 weeks on ventilator, vancomycin • Swollen painful right leg • Duplex scan
Case presentation (8) • DVT right leg • IV heparin • Rapid drop in platelet count on 3rd day of heparin • Heparin antibodies positive
Case presentation (9) • HIT (heparin induced thrombocytopenia) • New onset left hemiparesis • CT right parietal CVA • Patient treated with refludin • Gradual partial recovery from stroke
Case presentation (10) • Discharge to rehab 8 weeks post admission • 4 weeks later home with walker, visiting nurses, Physical therapy • Bills approaching the national budget of a small republic to be paid by the taxpayer (Medicare)
Case presentation (11) • On the first anniversary of his rupture walks into the surgeons office under his own power! • Four years later he is awarded $1,300,000 by a jury of his peers for negligence…on the part of his primary care provider!
Abdominal Aortic Aneurysm • Atherosclerosis • Genetic predisposition (weakening vs. occlusion) • Marfan’s, Ehlers-Danlos • Infection (Syphilis, salmonella, others)
Abdominal Aortic Aneurysm: Epidemiology • 15,000 Deaths per year USA • 13th leading cause of death in USA • 1.8-6.6% of patients in Autopsy series! • Strong male predominance 3:1 - 8:1 • Racial distribution Whites > Blacks
Increasing Incidence of AAA • Age-adjusted mortality rates for AAA increased 2.6-fold from 2.62 deaths per 100,000 in 1981 to 6.82 per 100,000 in 2000. • Hospital admissions for AAA also rose threefold, with increases in both elective admissions (from 3.05 to 7.80 per 100 000) and emergency admissions (from 7.44 to 11.23 per 100 000). (Data from Scotland) • Br J Surg 2003 Dec;90(12):1510-5BestVA; Price JF; Fowkes FG
AAA: Genetic predisposition • 15-20% AAA patients have 1st degree relative with AAA • 11.6x more common in persons who have 1st degree relatives with AAA • Duplex 25% males and 7% females have AAA if 1st degree relative has AAA • 69% risk of AAA in offspring of women with AAA! • Females rise from 14% to 35% in affected families
AAA: Genetic predisposition • Multifactorial inheritance • Though several “suspects”, specific genes not identified. • There are clearly “host factors”: patients have the same risk factors and demographics as patients with occlusive disease
AAA: Associated conditions • Emphysema: frequent association, and emphysema is the strongest independent risk factor for rupture of a known AAA • Destruction of elastin matrix in lung and aortic wall may have a common cause (e.g. alpha 1 antitrypsin deficiency) • 2x increase in inguinal hernias
Initial Diagnosis of AAA • 38% patients AAAs initially detected by PE • 62% found incidentally on x-ray studies done for other indications • AAAs detected by PE had lower BMIs but there was no difference in AAA size • 43 % of AAAs detected on radiologic examination had palpable AAAs that should have been detected on PE. • 23% AAAs were not palpable on preoperative PE, even when the diagnosis was known. • Obese patients had only 15% of AAAs detected by PE, and only 33% were palpable. • Role of physical examination in detection of abdominalaorticaneurysms. Surgery 1995 Apr;117(4):454-7 ChervuA; Clagett GP; Valentine RJ; Myers SI; Rossi PJ
AAA Examination • Physical Exam: Specific exam for AAA! • Deep palpation • ABOVE umbilicus • LEFT of midline • continuous over several heartbeats • AAA NOT detected on exam for tenderness or lower abdominal masses!
AAA Diagnosis • Ultrasound: low cost, reliable, fast, safe • Poor imaging above renals • CT: Excellent Dx, now able to “map” for surgery • MRI/MRI: Little if any advantage over CT • Angiogram: not optimal test for diagnosis, excellent for pre-op “mapping” • Flat Plate/KUB: Incidental finding of AAA
Indications for Repair • Size: 5.5 cm (NEJM) 346:1437-1444. 2002.Immediate Repair Compared with Surveillance of Small Abdominal Aortic Aneurysms • Lederle, Wilson, Johnson et.al. • 5.0 cm still used in common practice by many surgeons • Rupture (“Leak”) • Symptoms: abdominal or back pain, to groin in some cases. Tenderness of AAA
AAA: Risk of Rupture • Emphysema, smoking, hypertension increase liklihood of rupture (Cronenwett 1985) • Law of LaPlace T = Pr/2 • Larger Aneurysm more likely to rupture • <4cm: 2% rupture over 5 years • >5 cm 25-41% rupture over 5 years • 6 cm rupture rate ? 50% in 5 years
AAA: Influence of size NEJM.Powell and Greenhalgh 348:1895, 2003 The analysis is based on information from 1792 men and 465 women with abdominal aorticaneurysms
AAA: Treatment Options • Observation: Small aneurysms < 5 cm • Repair • Open surgical repair • Endovascular (“stent-graft”) repair
Surgical repair • 3-5% mortality (elective cases) • small risk of MI, pulmonary complications, renal failure, limb ischemia, hemorrhage, colon ischemia, etc • Repair effectively permanent
Endovascular repair • Quick recovery, less trauma, possibly lower mortality • “Endoleaks” about 30% need further procedures • Requires very tight follow-up • Expensive procedure
Open Health status predicts ability to withstand surgery Health status predicts chance of 5-10 yr survival “good” Likely to be difficult to maintain follow-up Renal “cuff”, iliacs preclude EVAR Endo (EVAR) Unusual risk for open surgery Limited life expectancy Likely to be compliant with follow-up “Friendly” anatomy of renal “cuff” and iliac arteries Endovascular vs. Open Repair
Blankensteijn, de Jong, Prinssen, et. Al. Two-Year Outcomes after Conventional or Endovascular Repair of Abdominal Aortic Aneurysms NEJM 2005. 352:2398-2405 351 Patients randomized to Open Surgery vs. EVAR Two year survival: Open 89.6% EVAR 89.7% Complication Free Survival 65.9% 65.6% Conclusion: “The perioperative survival advantage of endovasuclar repair over open repair is not sustained after the firstpostoperative year”
The two year survival after elective repair of an Abdominal Aortic Aneurysm is therefore about 90%. In contrast, what is the outlook for a ruptured abdominal aortic aneurysm?
Complications of Ruptured AAA • Hemorrhage and shock • Renal Failure • Anoxic Encephalopathy • Ischemic Colitis (30%) • Limb ischemia • Pulmonary failure • Countless others
As elective repair of aneurysms has become safer and more routine, there has been little improvement in the outcome of ruptured aneuryms repair • We therefore want to “steer” all our patients toward elective repair, whether open or endovascular
This becomes a challenge of our diagnostic efficiency: can we identify all (or nearly all) AAA prior to rupture? • This requires evaluation of the general population • Testing of the general population is referred to as “screening” for a disease
Screening tests accepted in the medical community • Mammography • Papinicolau smears (“PAP”) • Prostate Specific Antigen (PSA) • Stool hematest and sigmoidoscopy
Data regarding screening for AAA (Ultrasound) • Lancet. 2002;360:1531-1539 “Multicentre aneurysm screening study (MASS): cost effectiveness analysis of screening for abdominal aortic aneurysms based on four year results from randomised controlled trial” • Routine ultrasound screening of men older than 65 years for abdominal aortic aneurysm (AAA) reduced aneurysm-related mortality by 50%
Data regarding screening for AAA (Ultrasound) • The cost-effectiveness of a "quick-screen" program for abdominalaortic aneurysms. Surgery 2002 Aug;132(2):399-407 (ISSN: 0039-6060) Lee TY; Korn P; Heller JA; Kilaru S; et.al.
Lee TY; Korn P; Heller JA; Kilaru S; et.al. Screening for AAA was cost-effective with a CER (Cost Effectiveness Ratio) of $11,215. Society usually is willing to pay for interventions with CER of less than $60,000 (eg, CER for breast cancer screening, $16,000). The “quick screen” improved the CER to $6850. Moreover, screening populations with increased prevalence of AAA (eg, male, patients with family history) further improved the CER. Our analysis demonstrates that ultrasound screening for AAA should be offered to all males above the age of 60. Widespread screening for AAA should be adopted and reimbursed by Medicare and other insurers.
Meta-analysis of Mortality Associated with Abdominal Aortic Aneurysms in the Abdominal Aortic Aneurysm Screening Trials US Preventative Services Task Force Screening for Abdominal Aortic Aneurysm: A best evidence systematic review. Ann Int Med 2005; 142:203-211
Meta-analysis of All-cause Mortality in theAbdominal Aortic Aneurysm Screening Trials US Preventative Services Task Force Screening for Abdominal Aortic Aneurysm: A best evidence systematic review. Ann Int Med 2005; 142:203-211
U.S. Preventive Services Task ForceScreening for Abdominal Aortic Aneurysm: A Best-Evidence Systematic ReviewConclusion: For men age 65 to 75 years with any tobacco exposure, AAA screening reduces AAA-related mortality.Ann Intern Med 2005;142:203-11
U.S. Preventive Services Task ForceScreening for Abdominal Aortic Aneurysm: A Best-Evidence Systematic Review • USPSTF is a division of the US Department of Helth and Human Services • This recommendation will likely become a “standard of care” • Screening for AAA is everyone’s responsibility
Screening for AAA:Current Medicare Policy • Men over 65 with any smoking history • Single screening ultrasound • Must be ordered at initial “Welcome to Medicare” examination • Patients with Family History of AAA • (Exam my be ordered in any patient with suggestive physical findings, or known AAA
Second Case • 72 year old obese man comes to office • Followed annually by primary physician • History of BP, smoking and COPD
Second Case (2) • Screening Ultrsound performed • note thrombus in aneurysm
Second case (3) • Patient undergoes careful cardiac “clearance” evaluation • Patient has CT angiogram to evaluate anatomy for open vs. EVAR approach
Second Case (4) • Undergoes aneurysm repair • Discharge without complication • Resumes full activity over 3-4 weeks • (faster if done EVAR)