Download
1 / 38
380 likes | 629 Views
Molecular basis of Chronic Myelo-Monocytic Leukemia. Madrid, April 5 th , 2013. Overview. Disease definition & causes of death Genetic mutations Frequence Clonal architecture GM-CSF hypersensitivity Abnormal gene expression w/o mutation

E N D
Molecular basis of Chronic Myelo-Monocytic Leukemia Madrid, April 5th, 2013
Overview • Disease definition & causes of death • Genetic mutations • Frequence • Clonal architecture • GM-CSF hypersensitivity • Abnormal gene expression w/o mutation • Prognostic significance of gene mutation / deregulation • Impact on current disease management
CMML a disease defined by one positive criteria Clonal (oligoclonal?) disease of the HSC with monocytosis • Monocytosis (> 1 G/L) that persists for at least 3 months • NOT a CML Lack of Philadelphia chromosome Ph1 or BCR-ABL • - NOT a MLN-EoLack of PDGFR/FGFR rearrangement and eosinophilia • NOT an AML Blood and bone marrow blast cells < 20% • - In most cases : cell dysplasia, at least one cell line Tefferi A, Vardiman JW. Leukemia. 2008;22:14-22.
Persistant monocytosis > 1 G/L Why do these patients die?
The best recognizedprognostic factor is blast cell count Diagnostic feature Peripheral blood blasts Bone marrow blasts CMML1 < 5% < 10% • CMML2 5-19% • 10-19% Patients die in < 3 years from Progression to AML (< 25%) Consequences of cytopenias
Macrophages a-defensins HNP1-3 Lymphocytes « Monocytes » include a fraction of dysplastic granulocytes endowed with immunosuppressive properties Monocytes CD14+/CD24- CSF1 CD14-/CD24+ Immature granulocytes Droin N et al, Blood. 2010;115:78-88
Persistant monocytosis > 1 G/L Why do these patients die? Progression to acute leukemia Consequences of cytopenias Immune system deregulation
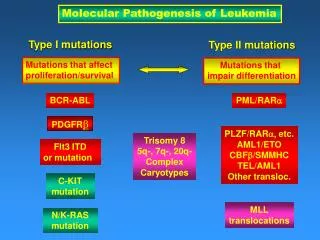
Molecular abnormalities in CMML cells 1 - Non specific cytogenetic abnormalities* 30-40 % 2 - Gene mutations (5-20 / patient) 100 % > 30 recurrently mutated genes 3 - Deregulated expression of genes (down, up) 100 % * Such E et al, Haematologica. 2011;96:375-83
Gene mutations The 3 most frequently mutated genes are TET2 SRSF2 ASXL1 Studied in sortedperipheral blood monocytes Itzykson R et al, J Clin Oncol, 2013, in press Damm F et al, Leukemia, 2013, in press
TET2 mutations associate with SRSF2 mutations ASXL1 TET2 2 CMML groups ? TET2 +/- SRSF2 ASXL1 SRSF2 Itzykson R et al, J Clin Oncol, 2013, in press
Gene mutations in CMML Three frequently mutated genes TET2 +/- SRSF2 & ASXL1
51 47 43 19 8 4 1 0 1 2 3 4 5 6 The number of mutations in a survey of 19 candidate genes affects the prognostic ~70% cases
Single cell analysis of the mutations in 4 bone marrow cell compartments 19 genes sequenced on sorted CD14+ blood cells and HSC/MPP/CMP/GMP sorted Seeded at 1 cell per well Cultured for 12 days with cytokines Colonies picked up In each colony, mutation specific PCR
63 61 9 102 22 46 16 160 20 67 46 48 67 37 119 95 51 49 56 72 10 49 32 93 70 28 100 80 60 40 20 0 # 537 # 500 # 428 # 497 # 654 # 536 # 531 # 518 # 507 # 501 # 462 # 516 # 550 # 632 # 495 # 498 # 586 # 644 # 759 # 736 # 658 # 524 # 743 # 514 # 731 # 662 Early clonal dominance specifies CMML among myeloid neoplasms HSC : CD34+/CD38-/CD90+ Black 0 mutation Yellow 1 mutation Orange 2 mutations Red 3 mutations
TET2 SRSF2 KRAS Clonal architecture in CMML (1/3) • Early clonal dominance in HSC • Linear acquisition of mutations, starting with epigenetic and splice genes • Growth advantage to the more mutated cells with differentiation Itzykson R et al, Blood. 2013 Jan 14.
Clonal architecture in CMML (2/3) Growth advantage to the more mutated cells with differentiation
Clone 4 N = 7 Clone 1 Clone 2 Clone 3 N =10 N = 1 N = 73 Clone 5 N = 9 homozygous homozygous heterozygous TET2 TET2 TET2 homozygous TET2 U2AF35 U2AF35 U2AF35 U2AF35 BFSP2 BFSP2 BFSP2 BFSP2 TRAPPC6B TRAPPC6B TRAPPC6B TRAPPC6B CTTNBP2 CTTNBP2 CTTNBP2 CTTNBP2 MYLK MYLK MYLK MYLK heterozygous KRAS heterozygous KRAS homozygous KRAS ASAP1 ASAP1 ASAP1 ADCY10 ADCY10 ADCY10 ATP2C2 ATP2C2 ATP2C2 CEP63 CEP63 CEP63 HECW2 HECW2 HECW2 SIPA1L2 SIPA1L2 SIPA1L2 SMOC2 SMOC2 SMOC2 SH2B3 SH2B3 CTCF CTCF Clonal architecture in CMML (3/3) Exome sequencing in blood leukemic cells (16 variants :14 SNP, 2 indels) Single cell analysis in CD34+ cells KRAS wildtype KRAS homozygous Linear accumulation of mutations with some branching through HR
Clonal architecture in CMML Early clonal dominance Mostly linear acquisition of mutations Some branching due to mitotic recombinations Growth advantage to the most mutated cells Limited effect of current therapeutic approaches
Early dominance of TET2 mutations may participate to the differentiation bias 13 TET2mutchronic myeloid malignancies (8 JAK2V617F MPN, 5 MDS) CD34+/CD38-P=0.006 CD34+/CD38+ P=0.08
CD34+/CD38- CD34+/CD38+ Early dominance of TET2 mutations may participate to the differentiation bias ns * 4.0 3.0 2.0 1.0 0.0 (CD33+) GPA- / GPA+ Sh:TET2 Sh:TET2 Sh:SCR Sh:SCR Cord Blood CD34+
Proposed model to distinguish CMML from other chronic myeloid neoplasms CD34- CD34+/CD38- CD34+/CD38+ CMML Additional mutations? Different HSC of origin? Stochastic? Clonal Expansion TET2 gene mutation Other chronic myeloid neoplasms Myeloid Differentiation
Four parameters that affect the phenotype in chronic myeloid diseases The mutated gene SF3B1 and ring sideroblasts The altered pathway Signaling genes and proliferative forms of CMML The allele burden JAK2 in ET versus PV The early / late amplification TET2 and monocytosis
JMML is a RAS disease Hypersensitivity of progenenitors to GM-CSF Loh ML. Br J Haematol. 2011;152:677-87. Germline 10% Neurofibromatosis (NF1) Noonan syndrome (PTPN11, CBL) Somatic 90% Inactivating homozygous mutations in PTPN11, NF1, CBL Activating mutations in NRAS, or KRAS Usually only one mutation / patient by WGS
In CMML, hypersensitivity of GM-CSF is inconstant Serum-free + SCF GM-CSF 10 ng/mL Mutation in a signaling gene NRAS, JAK2, CBL 6/7 cases 3/13 cases Itzykson R et al, unpublished
GM-CSF hypersensitivity Heterogeneous (contrary to JMML) Mostly linked to mutations in signaling genes
n=9 n=9 4 Ctrl * D/D 3 n=12 n=20 2 ** Monocytes (k/mm3) n=12 n=23 n=11 n=23 1 0 1 cm 1-13 14-26 27-39 ≥40 Weeks Ctrl D/D 3% 44% 51% 1% Mac1-Alexa647 Gr1-FITC In the mouse, deletion of tif1gin myeloid cells (Transcription Intermediary Factor 1 g) induces a CMML phenotype Peripheral blood Spleen Ctrl D/D Aucagne R et al, J Clin Invest. 2011;121:2361-70
-139GGGAGGACGTCCGTGCGTACGTGCGCGTGCCGCAACCGCCCTCCTTCAAACGCGCGACGCG unconverted 35% of patients -139GGGAGGAYGT TYGTGYGTA YGTGYGYGTGT YGTAAT YGTTT TT TTTTAAA YGYGYGA YGYG Control TIF1g low TIF1g normal expression (Subset # 1) (Part of subset # 2) non methylated methylated TIF1ggene promoter is methylated in 35-40% of CMML Aucagne R et al, J Clin Invest. 2011;121:2361-70
120 Ctrl Dec. 100 80 Before treatment After 5 cycles Tif1g mRNA level 60 -92AAATGTGTGATGTGAGGGTGGGGGCGCCGCGTGCGTGTGTG CC C C 40 Before decitabine TIF1g 170 20 HSC70 72 0 Cycles -92AAATGTGTGATGTGAGGGTGGGGGTGTTGTGTGTGTGTGTG After decitabine 0 15 5 7 TIF1gexpression increase in CD14+ cells as a biomarker of HMAefficacy Aucagne R et al, J Clin Invest. 2011;121:2361-70
1.0 0.8 0.6 0.4 0.2 0.0 300 250 Normal TIF1g 200 Cumulative probablility of survival 150 Low TIF1g mRNA expression (relative) 100 50 0 6 12 18 24 30 Months 0 Control Subset # 1 Subset # 2 TIF1gexpression level does not predict decitabine efficacy Braun et al, Blood. 2011;118:3824-31.
Elevated CJUN and CMYB levels are negative prognostic factors 1.0 0.8 0.6 0.4 0.2 0.0 1.0 0.8 0.6 0.4 0.2 0.0 CMYB CJUN Low Low Cumulative probablility of survival High P = 0.06 P = 0.01 High 0 6 12 18 24 30 0 6 12 18 24 30 Months Months Braun et al, Blood. 2011;118:3824-31.
CMML: deregulated gene expression Up cJUN cMYB Down P15/INK4b – 50% TIF1 g – 40% miR-150 No prognostic impact Prognostic impact
100 80 60 40 20 0 100 80 60 40 20 0 Overall Survival (%) wildtype wildtype AML-free Survival (%) mutated mutated 187 187 134 134 84 84 50 50 19 19 5 5 187 187 126 126 77 77 47 47 18 18 5 5 125 125 68 68 29 29 10 10 6 6 1 1 125 125 56 56 23 23 9 9 6 6 1 1 0 0 12 12 24 24 36 36 48 48 60 60 0 0 12 12 24 24 36 36 48 48 60 60 ASXL1 mutations have a negative prognostic impact Univariate analysis ASXL1 : P < 0.0001 also SRSF2 : P = 0.03 CBL : P = 0.003 IDH2 : P = 0.03 Itzykson R et al, J Clin Oncol, 2013, in press
A simplified prognostic score that includes ASXL1 mutations Validation (MLL) :165 Training (GFM) : 312 Low Int High Low Int High Absence 0 0 0 0 0 Presence 3 2 2 2 2 Low < 4 Intermediate 4-8 High >8 Hyperleucocytosis (>15) Age (>65) Anemia Thrombocytopenia (<100) ASXL1 mutation Itzykson R et al, J Clin Oncol, 2013, in press
Molecular characterization of CMML in clinical practice To refine the diagnosis BCR-ABL PDGFR/FGFR KIT To capture prognostic informations ASXL1
Which molecular analyses ? Monocytes > 1 G/L Eliminate BCR-ABL Others ASXL1, Complex Karyotype Eosinophilia PDGFR / FGFR Mast cells KIT Yes (MLN-Eo) Imatinib Yes (SM) TKI? Yes HSCT?
Leucocyte count < 13 G/L > 13 G/L IPSS Poor prognostic factors 0 ou 1 > 1 Yes No Best supportive care Hydroxyurea HSCT HMA HSCT HMA Which therapeutic proposal?
1 - CMML : a disease of the HSC in whichgene mutations accumulate, mostlylinearly, and the mostmutatedcellsaccumulatewithdifferentiation. 2 - High number of geneticabnormalitieswith mutations inTET2, SRSF2 and ASXL1 being the mostprominent. 3 - Mutations in signalinggenes and early clonal dominance of TET2 mutations favor GM amplification. 4 – Treatment of poorprognostic CMML: ABMT (rarelyfeasible) and hypomethylating agents 5 – Molecular informations maybetter guide the therapeuticchoice in comingyears, with ASXL1 mutations affectingoutcome
Haematopoietic stem cell Lympho-myeloid progenitor cell lymphoid progenitor cell MEP CFU-GM BFU-E CFU-MK CFU-E CFU-M CFU-G CFU-T CFU-B erythro MGK platelet monocyte granulocyte T cell B cell NK red blood cell Gustave Roussy, Villejuif, France Raphael Itzykson Nathalie Droin Hana Raslova Margot Morabito François Delhommeau Philippe Rameau Cédric Oréar Guillaume Meurice William Vainchenker Olivier Bernard Marseille, France Daniel Birnbaum Véronique Gelsi-Boyer Lille, France Aline Renneville Claude Preudhomme Cochin, France Olivier Kosmider Michaela Fontenay Southampton, GB Claire Hidalgo-Curtis Nicholas Cross Dresden, Munich, Germany Uwe Platzbecker Thorsten Haferlach Suzanne Schnittger Groupe Francophone des Myélodysplasies P. Fenaux And all GFM clinical teams