Download
1 / 54
560 likes | 865 Views
THE CHEST EXAMINATION. Szymon Wcisło. Medical University of Lodz General Surgery and Thoracosurgery Clinic Military Teaching Hospital No. 2 Lodz, Zeromskiego Street No. 113. The regions of the chest.

E N D
THE CHEST EXAMINATION Szymon Wcisło Medical University of Lodz General Surgery and Thoracosurgery Clinic Military Teaching Hospital No. 2 Lodz, Zeromskiego Street No. 113
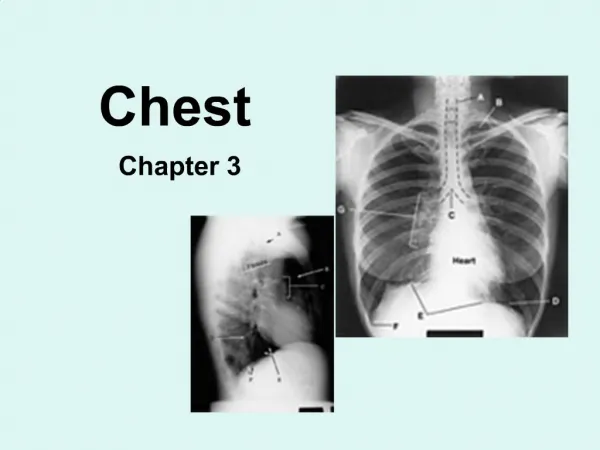
The regions of the chest • The surface of chest consists of some smaller regions which we can name similiar to the nearest points of the chest. • We can describe these regions on the front and back of chest.
Lines of the body • These lines are usefulness to describe localisation of some disorders and physiological symptoms which we can investigate in the chest.
Respiratory system • Trachea • Main bronchi • Right – wider, shorter and descendens more verticalythan left (foreign body most often run in right lung bronchial tree) • Left • LUNGS • Right – three lobes • Upper • Middle • Lower • Left – two lobes • Upper • Lower
Circulatory system • Heart • Four cavities • Right and left ventricles • Right and left atriums • Four valves • Bicuspid or mitralvalve • Aorticor semilunar valve • Tricuspid valve • Pulmonary valve
Circulatory system - heart • Apex – is the lowest part of the heart on the left side • This part of heart adheres to front wall of chest • We can see sometimes the apex beat – asthenic people
Clinical examination • Conduct an investigation • Always speek with patient – after and during physical examination • Conduct a physical examination • Inspection • Palpation • Percusion • Auscultation
Inspection • Age • Child • Adolescent • Young • Middle-aged • Elderly • Geriatric • Some diseases are conjugated with age
Inspection • Size • Short • Medium • Tall • Physical appearance • Thin / slim • Normal • Overweight / obese
Inspection • Body constitution = Size + Physical appearance • Pyknic (short + obese) • Normostenic (medium + normal) • Asthenic (tall + thin)
Inspection • Changes in skin colour • Normal • Bluishes / cyanosis – couse by some disorders of respiratory or circulatory system • Jundice – icterus • Pallor – shortness of breath • Redness – some skin inflammations, high fever
Inspection • Temperature • Normal 36,6°C • Subnormal • Elevated • High • Consciousness or unconsciousness • Perspiration – profuse or not • Swelling • Scars of previous operations
Inspection • Respiration • Abdominal – men • Thoracical – women • Asthmatic – status asthmaticus(bronchospasm – contraction of bronchi) • Laboured - dyspnoea • Shallow - hyperventilation • Tachypnoe – over 20 breaths per minute • Bradypnoe – below 14 breaths per minute
Inspection • Constitution of thorax • Barell chest – emphysematous chest • Rachitic chest • Chicken chest – sternum to front like birds • Funnel chest – shoe maker`s chest
Inspection • Skin lesions • Abscess • Cyst • Erythema • Macula • Nodule • Scar • Ulcer • Tumours – angioma, lipoma, papilloma, adenoma, cancer
Inspection • Erythema • Cyst • Ulcer • Tumour neoplasmaticus
Inspection • Sometimes we observe apex beat • Always we must observe typical localisation of: • Axillary lymph nodes • Lymph nodes over clavicle • Lymph nodes above clavicle • Breast – another exercises
Palpation • In this kind of examination we use our palm • All lesions detected in observation must be checked with palpation • Skin lessions always must be described with its diameters (cm)
Palpation • Tenderness • Rib fracture • Some skin lessions • Swelling • Pathological pulses on chest surface • Lymph nodes • Single or not • Enlarged or not • Sliding relative to tissues
Palpation Apex beat • This beat can be found in point localized in crossing: thefifth intercostal space and vertical line 2 cm medial to left midclavicle line • Norm: when the pulp of the forefinger covers this beat • If the apex beat is larger then forefinger pulp that can mean – fluid in pericardial cavity – heart tamponade
Palpation Size of forefinger pulp
Palpation Pectoral fremitus – the sensation felt by palpation • In summary of this examination we describe vocal fremitus like: • Symmetric • Unsymmetric • Some disorders of lungs can couse the unsymmetric pectoral fremitus for example • Pneumothorax (the presence of air or gas in a cavity of pleura) • Hydrothorax – fluidin the pleural cavity • Lung inflammation
Palpation • Symmetricaly in: • Regio pectoralis • Regio mammaria • Regio inframammaria
Palpation • Respiratory expansion • Inspected on back • Two hands examination • Symmetric or unsymmetric • Linea mediana posterior is the reference point
Percussion Finger percussion • Right middle finger tapping the left middle finger • In chest over the lungs we can hear: • Vesicular resonance – healthy lungs • Tympanic resonance – pneumothorax, pulmonary emphysema • Dull percussion sound – fluid in pleural cavity, inflammation, cancer,lung tissue without air
Percussion • We percuss symetricaly following points: • Front of the chest: • Second intercostal space near the sternum • Fourth intercostal space in midclavicle line • Sixth intercostal space in anterior axillary line • Over the clavicle • Back of the chest: • Over the scapula • Medialy to the scapula • Under the scapula
Percussion Respiratory movement • We check on back – scapular line • First patient inhales and stops the air in lungs and then we percuss the lung in vertical direction from up to down and stop when the percussion sound change from vesicular to dull – this is down inhaling border of examined lung • Secondary patient exhale and stops breathing then we percuss lung like when the patient inhale – exhaling border of examined lung • Norm: 2-6 cm
Percussion Respiratory movement Exhalation Inhalation
Percussion Lower border of lung • Vertical direction of percussion (up to down) • Vesicular resonance change to dull resonance sound • Patient in sitting positon • Patients always breath spontaneously
Percussion Heart percussion • Sometime we percuss the heart • In this examination we percuss the borders of heart • Irrelative (part of heart adhering to front wall of chest) • Relative (all shape of heart which we can percuss)
Percussion Relative borders of heart
Percussion Irrelative borders of heart
Percussion • Relative borders: • Upper border – third intercostal spaceor thirth rib • Left border – apex line(vertical line 2 cm medialy to left midclavicle line) • Right border – right sternal line • Down border – we don`t examine because of stomach fundus • Irrelative borders: • Upper border – fourth intercostal space or forth rib • Left border – apex line • Right border – left sternal line • Down border – fifth intercostal space
Auscultation • In this kind of examination we use stethoscope • We examine the lungs and heart • Over the lungs we can hear some kinds of murmurs or rales • Over the heart we can hear some murmurs
Auscultation Lungs auscultate • Symetrical examination • Norm over the lungs is vesicular murmur • Some inflammations or neoplasms can cause the more intensive and louder vesicular murmur • We auscultate the lungs in typical points of front and back chest wall • No murmurs sound sugests pneumothorax or fluid in the pleural cavity (hydrothorax)
IV intercostal space in midclavicle line II intercostal space near the sternum Auscultation
Auscultation VI intercostal space in front axillaryor midaxillary line Over the clavicle we check the murmur from lung apex
Auscultation In the middle of scapulas Over the scapula Above the scapula
Auscultation • Pathological lung murmurs which we can sometimes hear: • Moist rales • Coarse rales • Bubbling rales • Fine rales • Dry rales – like snoring • Crepitant rales – like walking on snow • Whistling rales – like whistle sound Like water gurgitation