Download
1 / 46
480 likes | 766 Views
CHEST. Begashaw M (MD). Introduction. Acute upper airway obstruction is a surgical emergency Infants are vulnerable more than adults. Upper Airway Obstruction. is an obstruction at or above the vocal cord characterized by inspiratory stridor. Etiology . Acquired

E N D
CHEST Begashaw M (MD)
Introduction Acute upper airway obstruction is a surgical emergency Infants are vulnerable more than adults
Upper Airway Obstruction is an obstruction at or above the vocal cord characterized by inspiratorystridor
Etiology • Acquired _Inhaled foreign body _Infection _Laryngeal spasm _Trauma to the neck _Vocal cord paralysis _External compression _Malignancy - laryngeal carcinoma • Congenital _ Laryngomalacia _ Laryngeal or tracheal web and stenosis _Subglottictumour _ Aberrant vessels _ Adenoids
CLINICAL FEATURES stridor(noisy breathing) suprasternal retraction tachycardia cyanosis
TREATMENT Tracheostomy Intubation Emergency cricothyroidotomy
CHEST INJURIES 25% of all trauma deaths are a result of chest injuries alone
CLASSIFICATION Blunt trauma - 85% of all chest injuries 2. Penetrating trauma -accounts for 15% -Stab &gunshot -results in hemothorax &pneumothorax
PATHOPHYSIOLOGY • Inadequate delivery of oxygen: • Ventilation-perfusion mismatch • Decreased tidal volume due to pain • Hypovolemiafrom bleeding • Mechanical obstruction due to tension pneumothorax& cardiac tamponade
INITIAL ASSESSMENT AND MANAGEMENT Ensuring adequate airway Ensuring adequate ventilation Control extreme hemorrhage &restore circulation
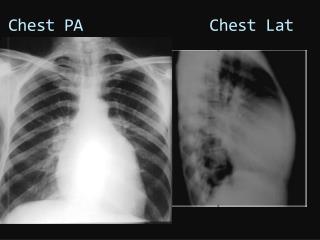
Chest wall injuries Simple rib fracture -Most common injury -less than three rib fractures other than first and second rib -pain, reduced motion during breathing and point tenderness -Confirm by Chest x-ray -Pain relief &chest physiotherapy
Major chest wall injuries Flail chest -paradoxical movement of a segment of chest wall -Fracture of four or more ribs at two points Diagnosis: paradoxical chest motion -Chest x-ray-multiple segmental fracture Treatment: Chest physiotherapy, Analgesia, Oxygen supplement Administer fluid only to restore hemodynamic stability Intubation for PPV
Fracture of 1st, 2nd rib & sternum considered to be major injuries causes associated injury to underlying structures like vessels or nerves
Lung contusion presents with bloody sputum upon coughing Diagnosis: Chest x-ray (parenchymal opacity immediately after injury &increasing in the next 24-48 hours Treatment: Pulmonary physiotherapy prevention of fluid load
Diaphragmatic rupture Mostly occurs on the left side diagnosis needs high index of suspicion Diagnosis: Insert NG tube Auscultatechest Chest x-ray - tube, loop of bowel or fluid level in the thorax Treatment: Immediate repair
PNEUMOTHORAX presence of air in pleural cavity TYPE: Open-chest wall wound communicate with external envt Tension-is a surgical emergency pressure compromises breathing/circulation Simple-not associated with compromised breathing/no breach of chest wall
CAUSE -Blunt &penetrating injuries MECHANISM -Fractured rib penetrating lung -Deceleration &crush disrupting alveoli -Sucking effect of negative intrapleural pressure
CLINICAL FEATURE decreased chest expansion tracheal shift hyper resonant percussion note decreased air entry If patient’s condition is stable, confirm by erect chest x-ray
TREATMENT remove trapped air through tube thoracostomy (chest tube) Incase of tension pneumothorax, insertion of needle at second intercostal space over the mid clavicularline of the same side relives the tension until chest tube insertion
HEMOTHORAX is collection of blood in the pleural cavity usually occurs from intercostalor internal mammary arteries Bleeding from parenchymal injury is nearly always self-limiting Massive Hemothorax is a bleeding of more than 1500ml in to pleural cavity
CLINICAL FEATURE history of trauma to chest Decreased air entry, dull percussion note Chest x-ray: costophrenicangle obliteration if more than 500 ml blood exists Ultrasonographycan reveal a small amount of fluid in the pleural recess
TREATMENT Chest tube insertion if sign of collection is visible on erect chest x-ray
EMPYEMA THORACIS is a collection of purulent fluid in the pleural space ETIOLOGY Pulmonary Infection_pnuemonia Trauma Aspiration of pleural effusion Extra pulmonary spread
CLASSIFICATION • Early (acute/exudative) phase Thin fluid , with PH less than 7, Glucose < 40 mg/dl & LDH >1000 IU/L - sub acute/fibro-purulent phase thicker pus with fibrin deposition loculationof pleural exudates • Chronic/organization phase fibroblast proliferation scar formation causing lung entrapment
Factors contributing to chronicity Delay in antibiotic treatment Inappropriate choice of antibiotics Failure of early intervention Presence of foreign body Failure to detect underlying lung pathology
MICROBIAL PATHOGENS In adults: Staphylococcus aureus Streptococcus pneumonia Streptococcus pyogens Immunocompromised Aerobic gram negative bacilli Fungal infection
Children: less than 6 month of age: Staphylococcus aureus 6 month-2 years of age: Staphylococcus aureus, Streptococci pneumonia and H.influenza 2 years- 5 years of age: H. influenza
DIAGNOSIS • Clinical -History of predisposing factors -Fever, pleuritic chest pain -Signs of pleural effusion -Signs of chronicity • Investigation 1. Routine-Hg, WBC, ESR 2.CXR-fluid level, meniscus sign 3. Fluid analysis a) Cloudy/purulent fluid pus b) Gram stain & culture c) AFB 4. Ultrasoundloculation/septation
TREATMENT _depends on – stage _ nature of primary infection _ source of contamination Antimicrobials Drainage of pus to achieve full lung expansion
Drainage Thoracentesis Closed tube thoracostomy Open tube drainage Rib resection &open drainage Thoracotomy&decortication
Prognosis depends _microbial agent, host defense, severity of disease, and duration /adequacy of antibiotics &drainage Mortality rate -healthy young -5% -immunocompromised/debilitated-40-70%
LUNG ABSCESS is a localized area of suppuration &cavitation in the lung with parenchymal necrosis
ETIOLOGY 1. Aspiration pneumoniacommonest 2. Primary necrotizing pneumonia 3. Bronchial obstructionneoplasm/FB 4. pulmonary trauma 5. systemic sepsis 6. Direct extension
MICROBIOLOGY -mixed aerobic &anaerobic bacteria DX sudden onset of cough productive of purulent sputum Fever with or without hemoptysis chronically sick, febrile with coexisting effusive finding
INVESTIGATION Sputum Gram Stain, Culture & sensitivity CXRconsolidation with or without cavitation&air fluid level
TREATMENT 1. Conservative: antibiotics, penicillin + metronidazolefor up to 6 wks 2. Operative: indication -failure of conservative -massive hemoptysis -thick or large cavity -suspected malignancy
COMPLICATIONS 1. Bronchogenic spread 2. Empyema 3. Cerebral abscess 4. Chronicity 5. Septicemia
PROGNOSIS uncomplicated -mortality rate <5% with prolonged &adequate abcs Complicated-mortality rate -75-90%