Download
1 / 15
150 likes | 326 Views
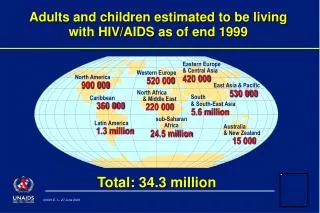
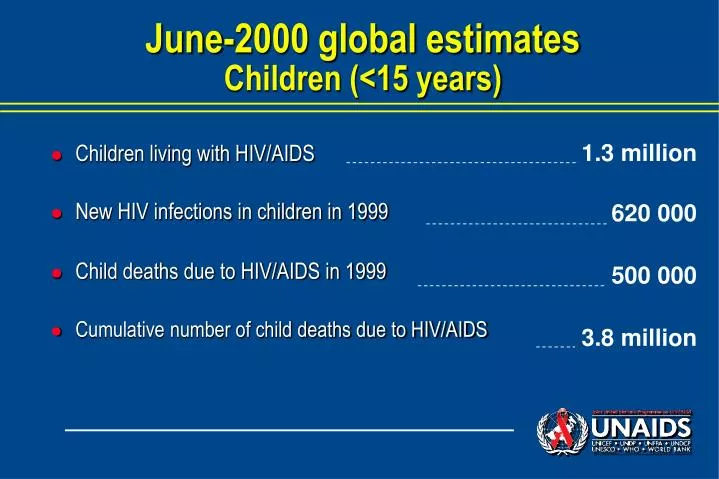
June-2000 global estimates Children (<15 years). 1.3 million 620 000 500 000 3.8 million. Children living with HIV/AIDS New HIV infections in children in 1999 Child deaths due to HIV/AIDS in 1999 Cumulative number of child deaths due to HIV/AIDS.

E N D
June-2000 global estimatesChildren (<15 years) 1.3 million 620 000 500 000 3.8 million • Children living with HIV/AIDS • New HIV infections in children in 1999 • Child deaths due to HIV/AIDS in 1999 • Cumulative number of child deaths due to HIV/AIDS
Estimated impact of AIDS on under-5 child mortality rates – Selected African countries, 2010 with AIDS per 1000 live births 250 200 150 100 50 0 without AIDS Botswana Kenya Malawi Tanzania Zambia Zimbabwe Source: US Bureau of the Census
Three integrated strategies to reduce paediatric AIDS Prevention of unwanted pregnancies (Family Planning) Prevention of Mother to Child Transmission (PMTCT) . during late pregnancy . during labor . through breast-feeding Primary HIV prevention in parents to be
Primary HIV prevention in the context of pregnancy • Information, Education and Communication programmes • Screening and treatment of Sexually Transmitted Infections • Condom promotion • HIV counselling NB: The risk of MTCT increases when the mother is infected during pregnancy or breastfeeding
Benefits of information, counselling and voluntary HIV testing for the community Widespread availability and use of counselling and voluntary HIV testing can : • Reduce fear, ignorance and stigma surrounding HIV • Stimulate a community response in support to those needing care • Contribute to an environment supportive of safer sexual behaviour • Reduce spillover of artificial feeding to HIV(-) mothers
Family Planning Strengthening • To prevent unwanted pregnancies HIV should never be used as a reason to pressurise women into having or not having children • To delay subsequent pregnancies For the health of mothers, WHO recommends a minimum of 2 years between pregnancies. • To replace the contraceptive effect of breastfeeding Avoidance of breastfeeding for PMTCT should not lead to rapid, unplanned subsequent pregnancy
Prevention of MTCT through antiretrovirals Mechanisms of action: • Ante and intra-partum regimen: Reduce viral load in mother ’s blood and genital fluids during pregnancy, labor and delivery • Post-partum regimen: Act as post-exposure prophylaxis (viral particles eventually transmitted during birth are eliminated)
Non-antiretroviral based intervention to prevent MTCT at birth • Ceasarian section : 50% risk reduction if performed before onset of labour • Avoidance of unnecessary invasive procedures (episiotomy, rupture of membranes…) : reduce infant contact with mother ’s infected blood and genital fluids • Vaginal lavage with chlorhexidine : may be protective in case of prolonged rupture of membrane (>4 hours before delivery) • Vitamin A supplementation : not effective to reduce MTCT
Prevention of MTCT after birth • Avoidance of breastfeeding = Replacement feeding: First 4-6 months: - Commercial infant formula - home made infant formula (diluted animal milk + sugar + vitamins) From 6 months to 2 years: - Enriched family foods • Exclusive breastfeeding + early weaning (as soon as replacement feeding is feasible and safe)
The variable risk of MTCT of HIV (with and without preventive interventions)
ARV regimen of proven efficacy Antenatal Postnatal Intrapartum ZDV long Infant ZDV short ZDV+3TC (1) Infant+Mother ZDV+3TC (2) Infant+Mother NVP Infant Birth 6wk PP 1wk PP Onset of labour 14wk 36wk Delivery
Balancing the risks of breastfeeding and formula feeding 12 months 24 months 6 months 14 wks 6 wks Child age Source: Nduati et al. JAMA 2000
A cascade of interventions Pregnant P ANC Pre-test counselling Test accepted Results given ARV initiated ARV completed Safer infant feeding Infections averted
Botswana pilot programme example First 8 months HIV+ Pregnant N=2900 P N=2900 ANC N=1650 Pre-test counselling Test accepted N=754 Results given N=638 ARV initiated N=435 232 ARV completed Safer infant feeding 174 Infections averted (estimated) 70
Botswana: Challenges and Responses Challenges : • Offer pre-test counselling to all women • Increase acceptability of HIV test Responses : • Train all mid-wives and doctors in HIV counselling • Develop communication programmes • Involve partners and/or other significant relatives