Download
1 / 53
530 likes | 566 Views
Explore the pathophysiology of side effects, ADR classifications, and patient risks with this lecture by Dr. R. van Eekeren. Learn how to prevent, recognize, and manage ADRs effectively in pharmacovigilance.

E N D
Author: Netherlands Pharmacovigilance Centre Lareb Version date: 14 Nov 2017 Content: This lecture describes Clinical Pharmacological aspects of ADRS, by R. van Eekeren, PharmD, The Netherlands. This lecture can be used for teaching key aspect 2,3,4: preventing, recognizing, managing ADRs.
Clinical pharmacology of adverse drug reactions Pharmacovigilance Course 2017 University of Groningen, The Netherlands Drs R (Rike) van Eekeren Pharmacist
Learning objectives • In this lecture, you learn to- apply the pathophysiologic principles that underlie to the occurrence of side effects • Characterize adverse drug reactions based different formats:- type A/B classification- DoTS classification • Discuss which patients have an increased risk of developing side effects
Dosis sola facit venenum “All substances are poisons; there is none which is not a poison. The right dose differentiates a poison and a remedy” Paracelsus (1493-1541)
Classification system 1 Exemple:Beta-blocking agents 1◦ dizziness, hypotension 2◦ Raynaud phenomena, dyspnoea in astma
Classification system 2: Type A/B B “Bizarre” • Idiosyncratic • Rare • Serious • Not detected in clinical trials A “Augmented” • Pharmacological effect • Dose dependent • Occurs frequently • Often detected in clinical trials Talbot J, Waller P. Stephen’sdetection of new adverse drug reactions. 5e editie, 2004. John Wiley &Sons Ltd. Chichester. P.92
Type A drug related Dose dependent Reversible Disappears after dose reduction or cessation of therapy Rechallenge often positive
Type B patient related Not dose dependent Sensibilization may be needed Reduction of dose often no effect on ADR Treatment is often needed Dechallenge positive
Type B patientrelated • Allergic / immunological reactionsExamples: Blood: seriousblood disordersLiver: hepatitisKidney: nephritisLung: pneumonia, alveolitis Skin: urticaria, angioedema, anaphylaxis • Otherpatient-related factors- Idiosyncrasy (undefinedsusceptibility)- Genetic factors (enzymedeficiencies, HLA-types)
AB types: No sharp distinction? When we do not know the exact mechanism:- Nausea in antibiotics type A, but unknown pharmacology? When the immune systems is triggered by toxicity mechanism- Toxic hepatitis Often, auto-immune component after initial hepatocellular damage In pseudo-allergy: allergic-like symptoms due to pharmacological effect- ACE-inhibitor induced angio-edema Time relationship? ADR’s after chronic use…Patient susceptibility? Why some patients develop ADR
Classification ADRs • Text • Text • Text • Text Mydriasis by amitriptyline Type? A(ugmented)
Classification ADRs Suppression of Hypothalamus-Pituitary- Adrenal cortex- axis (HPA) due to corticosetroids Type?C(hronic)
Classification system 3: DoTS • Do Doserelatedness • T Time relatedness • S Susceptibility
Dose relatedness • Effects of medicines are based on interactions between chemical substances, to which law of mass action is applicable • Even for immunological disorders like- Hay Fever!- Desensitisation- Allergic skin reactions
Dose relatedness Alternativeclassificationrelatestoreactionsthatoccur in • Supra-therapeutic doses (toxicdose) • Standard therapeutic doses (collateraleffects) • Subtherapeutic doses (allergicreactions)
Time relatedness Time-independent reactionscanoccur at any time; independent of theduration of the treatment treatthecauseifpossible • Change in concentration at site of action- Dose- Renalfunction- Drug interaction (kinetic)- … • Whenpharmacological response altersduetoothercauses- Comorbidity- Ageing- Drug interaction- …
Timing • Time dependentreactions • Rapidreactionsonlywhen a drug is administeredrapidly- Red man syndrome on vancomycin- administerslowly • First dosereaction. In particular, at first dose, notnecessarilytherafter- Hypotension ACE inhibitors, alfa-1-blockers precautionsfor 1st dose- Type I allergicreactions avoid re-exposure
Timing • Early reactions- early in treatment but then disappears through adaptation (tolerance)- Example: nitrate-dependent headache predictable, monitor, reassurance of patient • Intermediate reaction. Risk increases at first (days to month) and than diminishes- Hypersensitivity reactions II-IV- Venous thrombo embolism – antipsychotic drugs monitoring not needed after risk period withdraw drug if reaction develops susceptible population
Timing • Late reaction. The risk of the onset of the side effect increases with time- Osteoporosis in use of corticosteroids- Tardive dyskinesia at dopamine antagonists asses base-line function, monitor during treatment- Withdrawal reactions (like myocardial infarction after discontinuation of ß-blockers) withdraw slowly • Delayed reaction- Especially after prolonged use or repeated exposure- Increased risk of breast carcinoma after the use of estrogens in menopause avoud drug of screen; counseling patient
Individualsusceptibility Risks of an adverse reaction depends on various factors such as • Age • Gender • Genetic factors • Renal function • Hepatic function • Exogenous factors
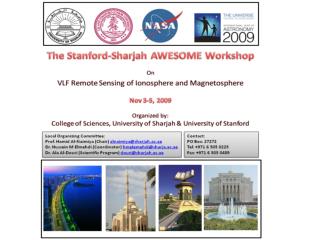
Drug therapy in young children Tan et al. MJA 2003
Adverse drug reactions in children • Different patterns compared to adults • Sometimes higher frequency- Liver failure and valproate- Stevens Johnson Syndrome and lamotrigine • Alterations in pharmacokinetics and pharmacodynamics
Pharmacokinetics in children DevelopmentalPharmacology – Drug Disposition, Action, andTherapy in InfantsandChildren Keams GL, Abdel-Rahman SM, Alander SW, Blowley DL, Leeder JS, Kauffman RE, NEMJ 2003
Pharmacodynamics • Increased or decreased sensitivity • Antihistamines: central stimulating effects • Benzodiazepines: paradoxical effects • Ketotifen: aggressive/hyperactive behaviour • Cyclosporin: High immunosuppressive response • Effects of growth and development
Drug therapy in theelderly • Aging process differs among individuals • Aging of various tissues may differ (within individuals) • Multiple morbidity • Polypharmacy (interactions) • Long term use of drugs • Compliance • Practical problems
ADRs in elderly 5-6% of all hospital admissions are preventable
ADRs in elderly JAMA. 2003;289:1107-1116.
Changes in function elderly Body composition Homeostasis e.g.- Temperature control- Orthostasis- Control of thirst Changes in tissues and organs (more vulnerable)
Pharmacokinetics: absorption Reduced motility of the oesophagus Local irritation of tablets (bisphosphonates) pH increase Slower gastric emptying Longer transit time intestine
Pharmacokinetics: distribution • Decrease in musclemass decrease in lean body mass • Lipophilicsubstances have greaterdistribution volume plasma concentrationinitally low • Hydrophilicsubstances have smaller distribution volume highertoxicityand more side effects • Albuminconcentrationhardly changes (decreasedbyunderlying disorders)
Elimination by liver Volume decreases, reduction of phase I reactions - Enzyme levels decreased - Especially CYP 1A2 and 3A4 Reduction of blood flow hepaticarteryand portal vein - Clearance of drugs with high first pass effect reduced - e.g. Propranolol 45% andmorphine 35%
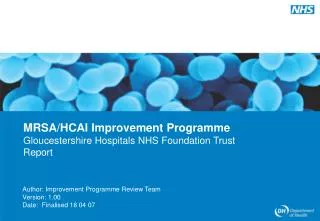
Elimination by kidney In about 1/3 of theelderly no deterioration of renalfunction In 2/3 changes occurdueto i.e.- Cortical area - Numberanddensity of glomeruli - Lengthand volume of proximaltubuli - Vascular changes
Kidney function and age Stevens et al. NEJM. 2006;354 (23): 2473
Pharmacodynamics • Changes may occur in:- Receptor density- Receptor structure- Propagation of signals • Sensitivity for various drugs- Increased (): psychiatric drugs, opioids, dopamine, agonists, parasympaticolytics- Decreased (): ß-blockers and insulin
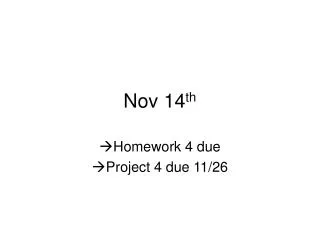
ADRs in elderly: risk of falling • Balance is complex mechanism controlled by- Vestibular system, Vision, Proprioception (orientation and movement), Muscle responses • Falling may occur due to- Cardiovascular effects: Orthostatic effects - Inadequate response due to vasodilatation - Reduction in function of baroreceptors - Insufficient fluid intake - α- or ß blocking agents, duiretics, ACE inhibitors, … • Psycho active drugs- Sedation, dizziness, confusion- Effect on extrapyramidal system- Muscle relaxants (benzodiazepines)
Psychoactive agents and falls Neth J Med2005;36:91-96
ADRs in elderly: thermoregulation • Problems in thermoregulation- Homeostasis for maintaining core temperature is changed- Ability to increase temperature (shivering) - Risk for hypothermia/poikilothermia • Antipsychotics may increase risk!
ADRs in elderly: cerebral function • Loss of neurons and receptors for cholinergic transmission • Additional neurologic disorders (i.e. stroke) • Anticholinergic drugs may influence cerebral function to large extent
Summary: DoTSand basic aspects • Dose- Pharmacological mechanism- Drug properties • Time • Susceptibility- Patient properties- Pharmacodynamics- Pharmacokinetics