Download
1 / 37
450 likes | 1.03k Views
NON INFECTIOUS PERIPHERAL ULCERATIVE KERATITIS [PUK]. A Clinical Approach DR. REKHA GYANCHAND Cornea consultant, Lions Eye Hospital BANGALORE. WHAT IS PUK ?. Potentially devastating Crescent shaped Juxtalimbal corneal stromal inflammation epithelial defect

E N D
NON INFECTIOUS PERIPHERAL ULCERATIVE KERATITIS [PUK] A Clinical Approach DR. REKHA GYANCHAND Cornea consultant, Lions Eye Hospital BANGALORE
WHAT IS PUK ? • Potentially devastating • Crescent shaped • Juxtalimbal corneal stromal inflammation • epithelial defect • Stromal infiltrate • Progressive stromal melting • If untreated necrosis of entire cornea
WHY IN PERIPHERAL CORNEA ? • Peripheral cornea - Unique anatomical & immunological features • Close to sclera / episclera / conjunctiva • Limbal capillary Arcade • Avascular central cornea • Associated with sub conjunctival lymphaticsafferent arm • IgM in periphery large • Langerhans cells • Reservoir of inflammatory cells • More susceptible to immunological damage
PATHOPHYSIOLOGY OF DAMAGE IN PUK Any inflammatory stimulus in peripheral cornea local cellular & humoral response complement activation vascular permeability chemotactic factors for neutrophils (C3a , C5a) neutrophil invasion Inflamm Of Conj proteolytic ,collagenolytic enzymes,leucotrienes destruction of collagen Collagenase Corneal thinning
CLINICAL PRESENTATION & DIAGNOSIS • 50% Of non infectious PUK due to collagen vascular disease (SLE, RP, PSS, RA,WG, PAN, GCA) • 34% of non infectious PUK caused by RA (Tauber et al) • PUK may be initial manifestation of WG & PAN • Moorens ulcer – local autoimmune disease with PUK
CLINICAL PRESENTATION &DIAGNOSIS - II • PUK due to CVD more in females • PUK due to Moorens more in males • Other causes include • Neoplasia • Rosaceae • Surgical trauma • Blepharitis • Inflammatory bowel disease
EXAMINATION IN PUK • Ocular • Systemic
OCULAR EXAMINATION Symptoms • Pain, epiphora, photophobia • pain if scleritis (RA, WG, PAN, RP) • pain without scleritis ( Mooren’s) • Decreased VA
EXAMINATION Examination of lids • Blepharitis • Telengiectasis (rosaecae) Posterior segment examination • Posterior scleritis • Vasculitis of CVD
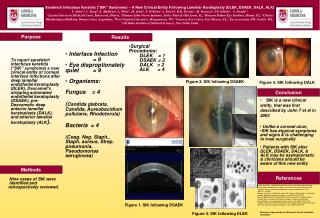
SLIT LAMP EXAMINATION-CORNEA • Crescent • Juxta limbal • Epithelial defect • Stromal yellow white infiltrates • Stromal thinning • Circumferential /central spread • Adjacent scleral / conjunctival inflammation
SLIT- LAMP EXAMINATION SCLERA • Associated necrotising scleritis systemic disease • In advanced cases- corneal/scleral melt
SYSTEMIC EXAMINATION • Thorough systemic history & examination mandatory • Important Questionnaire? • Weight loss, fatigue • Skin – facial rashes, ulcers, periungual infarcts(SLE) • Respiratory symptoms ( WG, SLE) • GI symptoms- pain diarrhoea ( SLE, WG) • Musculoskeletal symptoms- joint pain ( RA, SLE) • Neurological – seizures, Raynauds (WG, RP, SLE) • Genitourinary- hematuria ( PAN, SLE) • Swollen ear lobes (RP, SLE) • Deafness (WG) • Nasal ulcers/ bleeds ( WG) • Saddle nose ( WG, RP)
Differential Diagnosis Of PUK • Other Non Inflammatory Progressive Peripheral Thinning: • Terriens marginal degeneration • Pellucid marginal degeneration
TERRIENS MARGINAL DEGENERATION • Progressive , non inflam. thinning • No symptoms, V/A • Painless • Corneal epith intact • Begins superiorly • No stromal infiltration • Lipid deposition • Occasional adjacent conjunctival or scleral inflammation present • Can perforate
PELLUCID MARGINAL DEGENERATION • Bilateral,painless • Inferior corneal crescent thinning • Progressive • Clear zone of cornea • Epithelium intact • Adjacent conjunctiva no inflammation • Corneal ectasia above thinning • High against the rule astigmatism • Corneal topography
Laboratory Investigations For Non Infectious PUK • CHEST X-RAY • SINUSES (X-RAY / CT SCAN) • HEPATITIS B,C Ag • CBC • ESR • CRP • URINE ANALYSIS • RF • ANA (SLE/RA) • C ANCA (96% WG) • ANTI-ds DNA(SLE) • C3/C4 LEVELS • CIRCULATING IMMUNE COMPLEXES
LOCAL INVESTIGATIONS • Corneal scraping/culture • Conjunctival biopsy • Removes source of collagen • Diagnosis of CVD fibrinoid necrosis,granulomas,vasculitis • Diagnosis of Moorens justifies immune suppression in occult systemic disease
Treatment of Non Infectious PUK THERAPY MEDICAL SURGICAL LOCAL SYSTEMIC
LOCAL THERAPY Goals • Promote epithelial healing– stromal thinning • Control of inflammation • Collagenase inhibition– stromal thinning
Promote epithelial healing • Lubricating drops, gels • Avoid epitheliotoxic drugs ( aminoglycosides – tobra, genta; fluroquinolones—ciprofloxacin) • No role of topical antibiotics / antifungals unless secondary infection
Control of inflammation • No role of topical steroids/ NSAIDS • ( inhibits collagen synthesis—increases melt) • Use topical 1% medroxy progesterone • (good anti inflammatory, no collagen synthesis inhibition) • Can use topical cyclosporine 0.5- 1% • ( local T cell immune modulation) • Low dose topical steroids Lid hygeine only in marginal infiltrates with blepharitis ( staph antigen)
Other local medical treatment • Blepharitis: lid hygeine • Rosaecae: erythromycin ointment; metronidazole
SYSTEMIC THERAPY Systemic collagenase inhibitors • Tetracycline 250 mg QID • Doxycycline 100 mg OD • Systemic steroids + cytotoxic immunosuppressives
INDICATIONS FOR IMMUNE SUPPRESSION • PUK associated with proven CVD like RA, PAN, RP, WG, PSS, GCA, Churg-strauss angitis • If PUK associated with necrotising scleritis • If PUK unresponsive to aggressive conventional medical or surgical therapy
DRUGS USED High dose oral prednisolone 1- 1.5 mg / kg BW or Pulsed IV methyl prednisolone ( 0.5- 1g) started first as cytotoxic immunosuppression takes 4 – 6 weeks for action Drug of choice– oral cyclophosphamide ( 2 mg/ kg / day) adjust to clinical response, adverse effects
DRUGS USED • Methotrexate, azathioprine, cyclosporine-A • Methotrexate : DOC in RA ( 7.5- 12.5 mg / wk) • Azathioprine: 1.3 mg/kg/day • Cyclosporine-A:2.5-5mg/kg/day • Monitor CBC,LFT,renal function tests • Role of immunologist important • Good patient education: long term follow up systemic nature of disease
Surgical treatment Tissue adhesives ( cyano acrylate glue ) + BSL • Impending perforation / large thinning/ perforation size < 1-2mm • Delays disease process while patient is on immunosuppressives • infiltration of inflammatory cells
Surgical treatment • Conjunctival resection + superficial keratectomy + glue + BCL • Removes source of cytokines / inflammatory cells
Tectonic lamellar / full thickness corneal / scleral graft – Large Perforation w/ Uveal Prolapse
Simultaneous systemic immunosuppression very important or graft will also melt
LONG TERM MANAGEMENT Local disease healed • No inflammation • Epithelium intact • Vascularised Corneal pannus
LONG TERM MANAGEMENT • Long term follow up as relapses • Prolonged systemic immune suppression till underlying disease controlled even if EQ • Residual astigmatic correction– increases VA • Combination of LK +PK for visual rehabilitation done with full immunosuppression as surgery can trigger relapse • Cataract surgery when systemic disease under control & under systemic steroids
MOORENS ULCER • Distinct clinical entity in PUK • PUK not associated with CVD • ? Local auto immune disorder (altered corneal Ag) • ? Role of hepatitis C Ag
Distinguishing features • PUK unilateral / bilateral • Pain out of proportion • No scleritis • Typical overhanging central edge • More aggressive and early conjunctival resection and keratectomy advisable
Glue + BCL – if impending perforation & increased thinning Systemic steroids and immuno suppressives only if b/l moorens nonresponsive to local therapy Cyclophosphamide, methotrexate : DOC If Hep C Ag + : interferon alpha 2b ( 3 million units tri weekly SC inj – for 6 months
Conclusion.. • Non Infectious PUK is a potentially devastating disorder, can be the initial presentation of a serious collagen vascular disorder. Hence proper diagnosis and aggressive therapy could improve local and systemic morbidity.