Download
1 / 54
540 likes | 831 Views
Immunoglobulins: s tructure and f unction. Immunoglobulins. Definition : Glycoprotein molecules that are present on B cells (BCR) or produced by plasma cells (antibodies) in response to an immunogen. Immunoglobulin Structure. h eavy and l ight c hains d isulfide bonds

E N D
Immunoglobulins Definition: Glycoprotein molecules that are present on B cells (BCR) or produced by plasma cells (antibodies) in response to an immunogen
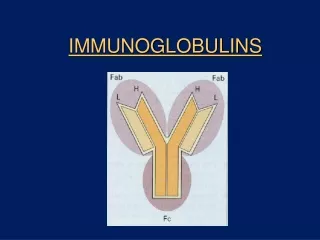
Immunoglobulin Structure • heavy andlight chains • disulfide bonds • inter-chain • intra-chain disulfide bond carbohydrate CL VL CH2 CH3 CH1 hinge region VH
disulfide bond carbohydrate CL CH2 CH3 CH1 hinge region VH Immunoglobulin Structure • variable andconstant regions • hinge region • domains • VL & CL • VH & CH1 - CH3 (or CH4) • oligosaccharides VL
antigenbinding complement binding site binding to Fc receptors placental transfer Immunoglobulin Fragments: Structure/Function Relationships
papain Immunoglobulin Fragments Structure/Function Relationships • Fab • antigen binding • valence = 1 • specificity determined by VH and VL • Fc • effector functions Fc Fab
pepsin Fc peptides F(ab’)2 Immunoglobulin Fragments: Structure/Function Relationships • Fab • antigen binding • Fc • effector functions • F(ab’)2 - Bivalent!
complex antigen antibodies complexed to complex antigen (A) High-affinity FcRs on the surface of the cell bind monomeric Ig before it binds to antigen. (B) Low-affinity FcRs bind multiple Igs that have already bound to a multivalent antigen.
the (Fab)2 fragment can - • detect antigen • precipitate antigen • block the active sites of toxins or pathogen-associated molecules • block interactions between host and pathogen-associated molecules but can not activate (role of Fc region) • inflammatory and effector functions associated with cells • inflammatory and effector functions of complement • the trafficking of antigens into the antigen processing pathways Why do antibodies need an Fc region?
Variability in different regions of the Ig determines Ig classes or specificity isotype allotype idiotype (Classes/subclasses) Sequence variability of H/L-chain constant regions Sequence variability of H and L-chain variable regions (individual, clone- specific) Allelic variants
Human Immunoglobulin Classesencoded by different structural gene segments (isotypes) • IgG - gamma (γ) heavy chains • IgM - mu (μ) heavy chains • IgA - alpha (α) heavy chains • IgD - delta (δ) heavy chains • IgE - epsilon (ε) heavy chains light chain types • kappa (κ) • lambda (λ)
Features of antibody-antigen interaction Valency: numbers of antigens / antibody Affinity: the strength of interaction between a specific antigen and one binding site of the antibody Avidity: sum of affinities of the binding sites of a a given antibody
S S S S S S S S S S S S S S S S S S S S IgA and pIgR are transported to the apical surface in vesicles s s s s s s s s s s C C C C C J J J J J C C C C C S S S S S S S S S S C C C C C C C C C C pIgR and IgA are internalised S S S S S S S S S S Polymeric Ig receptors are expressed on the basolateral surface of epithelial cells to capture IgA produced in the mucosa C C C C C C C C C C B B cells located in the submucosa produce dimeric IgA Secretory IgA and transcytosis ‘Stalk’ of the pIgR is degraded to release IgA containing part of the pIgR - the secretory component Epithelial cell
Antibody production during the primary and the secondary immune response level of antibodies secondary response against antigen A primary response against antigen A primary response against antigen B days napok Antigen A and B Antigen A
Antibody production during the primary and the secondary immune response
EFFECTOR FUNCTION OF ANTIBODIES Neutralization OpsonizationfollowedbyPhagocytosis ADCC Activation of complement (discussedlater)
Antibody Dependent Cellular Cytotoxicity (ADCC) NK CELL DEGRANULATION
MONOCLONAL ANTIBODIES versus POLYCLONAL ANTIBODIES
Ag Ag Ag Polyclonal antibody response Polyclonal antibody Immunserum Set of B-cells Activated B-cells Antibody-producing plasma-cells Antigen-specific antibodies
Monoclonal antibodies • product of one B-lymphocyte clone • homogeneous in antigenspecificity, affinity, and isotype - can be found in pathologic condition in humans (the product of a malignant cell clone) • advantages against polyclonal antibodies: antibodies of a given specificity and isotype can be produced in high quantity and assured quality. • therapeutic usage of monoclonals: • anti-TNF-α therapy in rheumatology, • tumor therapy
Possible use of monoclonal antibodies • Identifying cell types • Immunohistochemistry • Characterization of lymphomas with CD (cluster of differentiation) markers • Isolation of cells • Isolation of CD34+ stem cells for autologous/allogeneic transplantation (from peripheral blood!) • Blood group determination (with anti-A, anti-B, and anti-D monoclonals) • Identification of cell surface and intracellular antigens • Cell activation state • Targeted chemotherapy • CD20+ anti-B-cell monoclonals in non-Hodgkin lymphoma • Prevention of organ rejection after transplantation
Monoclonal antibodies as drugs? Mouse monoclonal antibodies may elicit an immune response upon administration in human subjects. (see immunogenicity-determining factors!) How can we solve this problem?
Human Mouse Humanized Evolution of monoclonal antibodies Chimeric Humanized antibodies are antibodies from non-human species whose protein sequences have been modified to increase their similarity to antibody variants produced naturally in humans.
mouse monoclonal antibodies immunization humanized mouse monoclonal antibodies immunization Human immunoglobulin transgenic mouse human monoclonal antibodies ENDANGERED SUBJECT PASSZÍV IMMUNIZÁLÁS PROTECTED SUBJECT serum antibody This is a case of PASSIVE IMMUNIZATION Immunesystemis notactivated prompt effect temporaryprotection/effect Immunoglobulindegradation
Monoclonals as drugs - Tumor therapy Monoclonals can be used for targeted chemotherapy of tumors. It is cell-type specific, but not specific to malignant cells! • Immunsuppressive monoclonals Cell-type specific immunsuppression
Monoclonals in tumor therapy • „Naked MAb”, unconjugated antibody • Anti-CD20 (rituximab – Mabthera/Rituxan, chimeric): B-cell Non-Hodgkin lymphoma • Anti-CD52 (campath – Mabcampath, humanized): chronic lymphoid leukaemia • Anti-ErbB2 (trastuzumab – Herceptin, humanized): breast cancer • Anti-VEGF (bevacizumab – Avastin, humanized): colorectalis tu. (+ Lucentis!) • Anti-EGFR (cetuximab – Erbitux, chimeric): colorectalis tu. (+ Vectibix, rekomb. humán!) • 2. Conjugated antibody • Anti-CD20 + yttrium-90 isotope (ibritumomab- Zevalin) • Anti-CD20 + iodine-131 (tositumomab – Bexxar)
Immunsuppressive antibodies 1. • Anti-TNF-α antibodies • infliximab (Remicade): since 1998, chimeric • adalimumab (Humira): since 2002, recombinant human • Etanercept (Enbrel) – dimer fusion protein,TNF-α receptor + Ig Fc-part • Not a real monoclonal antibody, no Fab end,the specificity is given by TNF-receptor! • Indications of anti-TNF-α therapy: • Rheumatoid arthritis • Spondylitis ankylopoetica (SPA - M. Bechterew) • Psoriasis vulgaris, arthritis psoriatica • Crohn-disease, colitis ulcerosa • (usually - still – not in the first line!)
Casestudy (Multiplemyeloma) • In 1989, a 55-year-old housewife, who had been in good health her entire life, • began to experience excessive fatigue. • Her physician did not find abnormalities on physical examination. • The blood sample revealed mild anemia; • red blood cell count was 3.5 x 106 / ml (normal 4.2-5.0 x 106 / ml), • white blood cell count was 3600 / ml (normal 5000 / ml). • The sedimentation rate of her red blood cells was 32 mm / h (normal <20 mm / h). • (Sedimentation is accelerated when fibrinogen or IgG content of the blood plasma • is elevated.) • The concentration of IgG was found to be 3790 mg / dl (normal 600 - 1500 mg / dl), • that of IgA 14 mg / dl (normal 150 – 250 mg / dl) and that of IgM 53 mg / dl • (normal 75 -150 mg / dl).
What happens with the B cells in myeloma multiplex? Healthy individual Myeloma multiplex
Case study (Multiple myeloma) • Electrophoresis of her serum revealed the presence of a monoclonal protein, which • on further analysis was found to be IgG with lambda light chains. normal serum serum from the patient • Radiographs of all of her bones did not show any abnormality. • No treatment was advised.
Case study (Multiple myeloma) • In April 1991 her serum IgG was 4520 mg / dl, and in January 1992 it was • 5100 mg / dl. By November 1992, her anemia had worsened and her red blood • cell count had fallen to 3.0 x 106 / ml. At the same time her white blood count had • fallen to 2600 / ml. • In December 1992, she experienced the sudden onset of upper arm pain and • headache. • Radiographs of the skull and the left upper arm showed ‘punched out’ lesions in • the bones.
Case study (Multiple myeloma) • She was treated with melphalan (methylphenylalanine mustard), corticosteroids, • and irradiation. Her symptoms improved. • In April 1993, further chemotherapy was given because of the persisting elevation • of her serum IgG. The treatment reduced her serum IgG level from 8200 mg / dl to • 6000 mg / dl. • In February and in May 1995, she was found to have pneumonia. She was treated • successfully with antibiotics. She recovered from this episode in the hospital and • remained fully active. She required blood transfusion for her anemia and complainedat times of bone pain. Her serum IgG was stable at 6200 mg / dl. • Although she was in relative good health as our case history ended, her outlook • for survival was very poor. Recently, bone marrow transplants have been used tocure patients with multiple myeloma. • /Myeloma proteins have played an important part in the history of immunology. • (Bence-Jones protein, subclasses of IgG, amino acid sequence of immuno- • globulin molecule)/
Questions She became anemic (low red blood cell count) and neutropenic (low white blood cell count). What was the cause of this? The proliferation of malignant plasma cells in the bone marrow crowded out blood cell precursors. This creates a limitation on space in the bone marrow.
As her disease progressed, she became susceptible to pyogenic infection; for example, she had pneumonia twice in a short period. What is the basis of her susceptibility to these infections? Although her serum IgG concentration is quite elevated, almost all the IgG is secreted by the myeloma cells and is monoclonal. In fact, she has very little normal polyclonal IgG and has been effectively rendered agammaglobulinemic by her disease. In addition, her white blood cell count is decreased and she has too few neutrophils (<1000 / ml) to ingest bacteria in the bloodstream and lungs effectively. A monoclonal immunoglobulin in the serum is called an M-component (‘M’ for myeloma). Is the presence of an M-component in serum diagnostic of multiple myeloma? No. M-component appear in the blood as people age. About 10% of healthy individuals in the ninth decade of live have M-component. This is called benign monoclonal gammopathy. Without bone lesions and presence of many malignant cells in the bone marrow, the diagnosis of multiple myeloma cannot be made. Some people have IgM M-components in their blood. This is due to another malignancy of plasma cells called Waldenström’s macroglobulinemia, which differs in many ways from multiple myeloma and is a more benign disease.