Download
1 / 49
500 likes | 1.26k Views
The Skinny on Atopic Dermatitis Robyn Morrissette, PA-C Division of Allergy and Immunology Pediatric Specialists of Virginia. No conflicts of interest to disclose. Learning Objectives: To understand how to recognize and diagnose atopic dermatitis

E N D
The Skinny on Atopic Dermatitis Robyn Morrissette, PA-C Division of Allergy and Immunology Pediatric Specialists of Virginia
Learning Objectives: • To understand how to recognize and diagnose atopic dermatitis • To learn the clinical presentation of atopic dermatitis • To review common treatments for atopic dermatitis • To review developing treatment for atopic dermatitis in the pediatric population • To review the association with food allergies.
Case: Julia 7 month old female • Referred to clinic by PMD for evaluation of a rash and to find the cause, concerned it is a food allergy • Rash started around 3mo and has worsened over last 3 months • Started on the cheeks initially but is spreading to trunk • Seems uncomfortable and itchy • Has been told not to bathe every day as this will make the skin worse
Case Report: Julia • Mom has been moisturizing with Aveeno twice a day • Given Hydrocortisone 2.5% to use twice a day sparingly and only for 1 week. • Medication worked but mom was nervous to use it again • Rash seems to get worse if Julia is upset • Rash seems worse if it is hot outside or if Julia is hot • Seems to have difficulty sleeping when the rash is really bad
What is Atopic Dermatitis? • Chronic pruritic inflammatory skin disease • Affects about 13% of children and about 7% of adults in the US alone • Also known as eczema • Often called the “itch that rashes”
What is Atopic Dermatitis? • Exact cause is unknown • Thought to be due to a “leaky” skin barrier • Do know there is an association with the Filaggrin gene and increased risk for AD • Also some link to substances that contain proteins called proteases – proteases break the link between the skin cells and make the skin barrier leaky
What is Atopic Dermatitis? • Sensitization to environmental allergens and food allergens commonly seen but is not a cause • Is an allergic spectrum disorder as patients with moderate to severe disease often have elevated serum IgE • About 70% patients have a positive family history of atopic diseases • Risk can increase to 3-5 fold if both parents have atopic disease
Clinical Presentation of Atopic Dermatitis • Presentation varies widely • Childhood onset begins early in life • About 50% in first year • About 85% by age 5 • Can persist into adulthood in anywhere from 20-50% of patients • Can have adult onset • Reported by about 26% of adult patients
Clinical Presentation of Atopic Dermatitis • Dry skin and severe pruritis • Erythematous maculo-papular rash • Vesicles that can have exudate and crusting (acute flare) • Dry, scaly, excoriated patches (more chronic lesions) • Lichenification (chronic) • Hyper/hypo-pigmentation
Clinical Presentation of Atopic Dermatitis • Excoriations at various stages of healing • Persistent fidgeting due to pruritis • Irritability • Insomnia due to pruritis at night • Decreased concentration secondary to itching and being uncomfortable
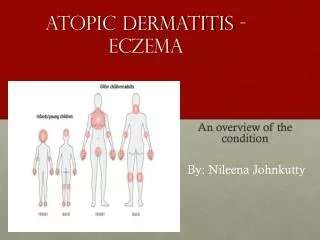
Clinical Presentation of Atopic Dermatitis • In infants to around age 2: Commonly starts on face and scalp. Sometimes on extensor surfaces. • Typically spares the genitalia/diaper area • Age 2 – teenager: Presents more on the flexor surfaces • Typical antecubital fossa and popliteal fossa presentation • Volar aspect wrists, ankles, neck • Adults: Continues on flexor surfaces and also on hands
Diagnosing Atopic Dermatitis • Clinical diagnosis based on history and presentation • Rule out other dermatologic conditions • Rule out rare immunodeficiency conditions such as hyper-IgE syndrome and Omenn syndrome • Eczema accompanied by other symptom such as failure to thrive, skin abscesses, cutaneous viral infection, chronic diarrhea • In adults need to rule psoriasis and cutaneous T-cell lymphoma
Diagnosing Atopic Dermatitis • Several sets of criteria have been developed • Hanifin-Rajka (H-R) criteria considered the gold standard • United Kingdom Working Party (UKWP) abridged version of H-R criteria, tends to work better for pediatric diagnosis • Not all allergist/dermatologist use a diagnosing criteria
Treatments for Atopic Dermatitis • Accepted for publication June 26, 2019 • Includes newer topical medications like Crisaborole (Eucrisa)
Treatments for Atopic Dermatitis • Treatment is daily given the chronicity of the disease • Multifaceted • Personalized to the patient and severity • Often requires review at follow up visits to ensure compliance
Treatments for Atopic Dermatitis • Atopic Derm myth #1: Baths make AD worse. • Every patient no matter severity gets daily care of basic management (bath and moisturizing) • Daily bath Soak and seal • 15-20 minutes warm, clean water • Infants/small kids place wash cloth over areas not under water and continue to wet • Older kids can do shower • Soaps do not have to be done daily. If used, use at end and rinse immediately then out of bath. • Pat dry • Apply emollients (Aquaphor or Vaseline)
Treatments for Atopic Dermatitis • Recommend moisturizing in the morning and at bedtime after bath. • Should do at least 1 more time mid-day/afterschool • Can be done as needed • Infants – easy to tell parents to do with diaper changes • Older patients can use non-fragranced lotion (CeraVe, Aveeno, Cetaphil, Eucerin)
Treatments for Atopic Dermatitis • Avoidance of triggers (allergens and irritants) • Fragrances • Wool • Temperature extremes • Foods • Soaps/detergents
Treatments for Atopic Dermatitis • Topical Medications • Topical corticosteroids (Hydrocortisone, Triamcinolone, Desonide, etc) • Topical calcineurin inhibitors (pimecrolimus and tacrolimus) • Phosphodiesterase-4 inhibitor (Crisaborole) • Systemic immunosuppressants (Cyclosporine, Methotrexate) • Injectable medications • Dupilumab • Oral antihistamines
Treatments for Atopic Dermatitis Topical Steroids • Atopic Derm Myth #2: Use steroids sparingly and only for 7 days and no more. • Topical steroids applied twice a day to flare • Use a thick layer of the medication • Prefer ointment over creams/lotions • Use lowest potency that still controls the symptoms • Use until area clears then 2-3 more days • Can use up to 14 days in a row before needing to take a break
Treatments for Atopic Dermatitis Topical Steroids • In some patients with severe atopic derm can do a daily preventive application of topical steroids • Typically done under supervision of Allergist or Dermatologist • Safe to use in infants • Side effect profile is mild if used appropriately • Side effect of topical steroids discoloration of the skin and thinning of the skin • Minimal absorption systemically if used appropriately
Treatments for Atopic Dermatitis Topical Calcineurin inhibitor • Includes Pimecrolimus and Tacrolimus • Approved in use for patients age 2 years and older • Popular for use on eyelid atopic dermatitis and hand dermatitis • Can use up to 14 days in a row • Side effect profile is mild if used appropriately • Most common side effect is redness initially at the application site improves with use • Can make you more photosensitive
Treatments for Atopic Dermatitis Topical PDE4 inhibitiors • Crisaborole (brand name Eucrisa) • Approved December 2016 • Ages 2 and older • Nonsteriodal topical ointment that inhibits PDE 4 (intracellular mediator of inflammation that degrades cyclic adenosine monophosphate) • Can be applied anywhere except in the eyes, in the mouth, or vaginally
Treatments for Atopic Dermatitis Topical PDE4 inhibitiors • Applied twice a day • No limitation in how long it can be used • Side effect profile is mild • Most common side effects include redness and pain at application • In our clinic majority of patients who come in on this medication have stopped if for these reasons
Treatments for Atopic Dermatitis Additional Therapies • Oral antihistamines to control itching • Cetirizine can be used as young as 6 months old • Hydroxyzine at bedtime to control itch and help sleep • Topical and oral antibiotics as needed for superinfection • Wet wrapping: Intense moisture therapy involving wrapping affected areas overnight for 5 nights • https://www.nationaljewish.org/conditions/eczema-atopic-dermatitis/eczema-treatment/wet-wrap-therapy
Treatments for Atopic Dermatitis Additional Therapies • Biologics: • Newest medication approved for treatment of moderate-severe atopic dermatitis • Dupilumab (Brand name: Dupixent) • Monoclonal antibody that targets IL-4 receptor alpha-chain subunit common to IL-4 and IL-13 • Injectable medication • Reduction of pruritis • Reduction in symptoms of anxiety and depression • Improvement in quality of life • Approved for 12 years and older • Done under supervision of Allergist and/or Dermatologist
Treatments for Atopic Dermatitis Additional Therapies • Bleach bathes • Phototherapy • Hospitalization for intense eczema care • Systemic immunosuppressants
Atopic Dermatitis and Food Allergies • Commonly see patients with AD have food allergies but as discussed above it is not the cause • Can be at increased risk for food allergies • LEAP study – risk factors included severe eczema • Increased risk of peanut allergy if not introduced early • NIH study
Atopic Dermatitis and Food Allergies • NIH guidelines regarding peanut introduction
Atopic Dermatitis and Food Allergies • Broad panel serum IgE or skin prick testing is not recommended in patients with eczema • Broad panel testing can lead to unnecessary food avoidances and potential development of food allergies due to avoidances • FARE blog post from December 2015 does a great job discussing research • http://www.foodallergy.org/about-fare/blog/new-research-on-food-allergies-and-atopic-dermatitis • History can help with difference between allergic reaction and food triggered eczema
Back to baby Julia… • Started daily eczema care plan including: • Daily bath • Frequent moisturizing with Vaseline or Aquaphor • Topical Desonide to face/neck flare ups and topical Triamcinolone to body flare ups • Cetirizine in the morning as needed for itching and Hydroxyzine at bedtime as needed for itching • Once the eczema was controlled addressed food allergy concerns • Skin testing negative to egg and peanut • Introduction at home
Sources Fishbein, A, Silverberg, J, Wilson, E, Ong, P. Update on Atopic Dermatitis: Diagnosis, Severity Assesment, and Treatment Selection. The Journal of Allergy and Clinical Immunology: In Practice. https://doi.org/10.1016/j.jaip.2019.06.044 Weston, W, Howe, William. Atopic dermatitis (eczema): Pathogenesis, clinical manifestations, and diagnosis. https://www.uptodate.com/contents/atopic-dermatitis-eczema-pathogenesis-clinical-manifestations Photos property of Dermnetnz.org
Sources Schneider, L, Tilles, S, Lio, P, et. al. Atopic Dermatitis: A Practice Paramater Update 2012 https://www.aaaai.org/aaaai/media/MediaLibrary/PDF%20documents/Practice%20and%20parameters/Atopic-Dermatitis-2013.pdf