Download
1 / 14

E N D
Cardiac Tamponade A Case Study
The background You admitted MB after a LIMA-LAD, SVG x2, initial vital signs were stable – HR 75, BP 114/73, CVP of 5, Cardiac index was 2.1 after 250 ml of albumin index was up to 2.3, pulses are present and easily palpable. There was good amount of urine in the OR and is doing well since they have come back. Hgb was 10.7. You have 3 blake drains to 2 pleuravacs, initial output was 70 out of your single chest tube and 60 out of the y’d chest tubes, both with good bubbling. Two hours later CI remains 2.3, you have given two more albumins (for a total of 750 ml), BP if 102/70, CVP 11, HR 82. Chest tubes put out 40 and 50 in the last hour, intermittent bubbling is present, patient is just starting to wake up, you are seeing some eye movement and random movement of extremities. Two hours later your HR is 105, BP is 90/61, CVP 23, CI 1.9, pulses are present but weak, chest tube output for the last hour is 5 and 5, and no bubbling is seen. You get your hgb back and it is 8.2.
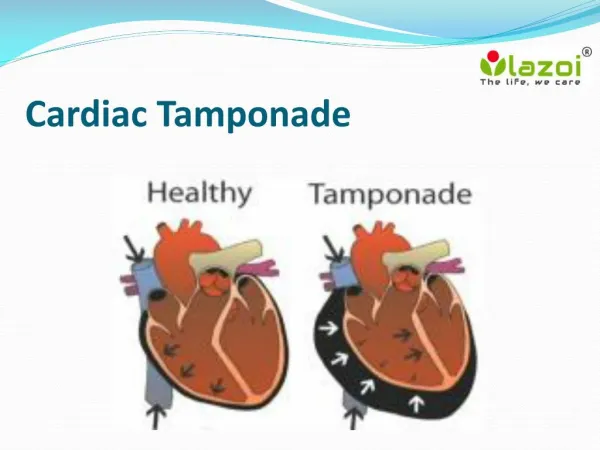
What do you think is happening? • The patient is likely experiencing a cardiac tamponade
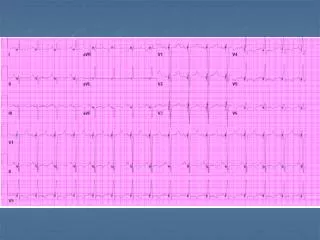
What is a test the physician might order and what will it show? • Sometimes a chest xray will be ordered, to check for a widened mediastinum.
What are some physical assessment findings that support the diagnosis of cardiac tamponade? • Distant heart tones, weak peripheral pulses, restlessness/confusion (if awake), JVD
What do you expect the physician to tell you? • They will be on their way in, either to take patient back to the OR or open their chest at bedside depending on stability of the patient upon arrival (they will probably tell you before heading in what their plans are). The goal will always be to get them to the OR so they are in a sterile environment upon opening the chest.
What do you need to do before physician arrives? • Notify the OR that the physician is on the way in, they either need to have OR ready or have someone assist at bedside). You can attempt to strip/milk the chest tubes to work clots out, sometimes turning patients side to side, or sitting them straight up, or making them cough helps bring clots further down in the tubes.
What could have prevented this? • The best thing to do to prevent tamponade is to turn patients side to side quickly, and always monitor your chest tubes and milk them as much as possible. Sometimes due to positioning of tubes, amount of blood loss, & status of coags there is just not much that is able to be done.
What signs help show that this is a tamponade? • Narrowing pulse pressure (normal 30-40), all of your heart pressures are starting to move towards ‘one’ number, decreasing urine, decreasing pulses.
What will happen to this patient if no interventions occur and why? • Patient will eventually go into multisystem failure (no urine, liver shock, etc) and code, leading to death. The heart is being squeezed from the outside so that minimal blood is actually being circulated.
How is the presentation of this patient different than a patient that walks into the ER with a pericardial effusion with tamponade and why are the situations different? • Typically a patient that comes into the ER with a cardiac tamponade, unless it is from trauma, shows similar symptoms, however that patient has had time to compensate for the decreased flow and it is not quite as an emergent situations. This is not saying that that patient is not critical, but there is usually a little more time before that patient is going to code. Typically you can rely on neuro symptoms more reliably with someone who has NOT just had surgery – after surgery you don’t know whether they are restless/confused because of anesthesia and pain medications or because of decreased flow.
The Nurses Role • The majority of items in the nurses role are in prevention of this happening: moving the patient and working with the chest tubes in order to prevent clotting. • Once this has occurred the nurses role shifts into organizing the patient and preparing them for a trip to the OR. • As this is occurring it is important to be monitoring the patient, checking frequent cardiac outputs, managing vasoactive drips, giving fluid (per orders)calling those who need called (OR team, Supervisor, Perfusionist) • If the patient happens to code before surgeon arrival – minimize compressions as much as possible. If compressions are required make sure to use bed pan/bath basin – something to distribute pressure across chest as much as possible • Often will look at the CXR – Radiologist often won’t look at mediastinum • Stay Calm!
Pictures Obtained from: • Cardiac tamponade picture: http://medical-dictionary.thefreedictionary.com/cardiac+tamponade • Widened Mediastinum: http://casereports.bmj.com/content/2011/bcr.03.2011.3956.abstract • Normal Chest X-ray: http://www.meddean.luc.edu/lumen/meded/medicine/pulmonar/cxr/atlas/cxratlas_f.htm • Chest tube striping/clogging : http://www.pleuraflow.com/clogging/