Download
1 / 26
350 likes | 897 Views
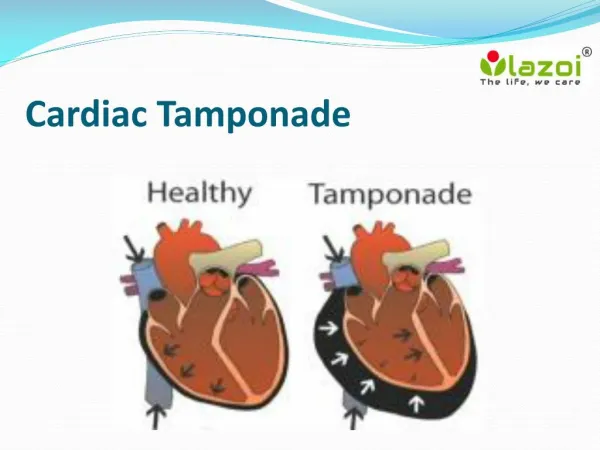
Cardiac Tamponade. Cardiac Tamponade. Normal amt of pericardial fluid = 20-50 mL Tamponade occurs when lg or rapidly formed effusions inc’d pressure in the pericardial space throughout the cardiac cycle

E N D
Cardiac Tamponade • Normal amt of pericardial fluid = 20-50 mL • Tamponade occurs when lg or rapidly formed effusions inc’d pressure in the pericardial space throughout the cardiac cycle • During inspiration, RV volume inc’s & in tamponade, the RV is unable to expand into the maximally stretched pericardium L-ward bulging of the interventricular septum dec’d LVEDV dec’d cardiac output & dec’d SBP during inspiration
Etiology of Cardiac Tamponade HIV, bacterial (incl mycobacterial), viral, fungal CA - Esp lung, breast, Hodgkin’s, mesothelioma Radiation tx Meds - Hydralazine, Procainamide, INH, Minoxidil Post-MI (free wall ventricular rupture, Dressler’s syndrome) Connective tissue dzs – SLE, RA, Dermatomyositis Uremia Trauma Iatrogenic – (eg, from TLC / PA Cath / TV pacemaker insertion, coronary dissection & perforation, sternal bx, pericardiocentesis, GE jnx surgeries) Other - Pneumopericardium (d/t mech ventilation or gastropericardial fistula), Pleural effusions Idiopathic
Clinical Presentation • Sxs • Chest Pain, dyspnea, near-syncope • Generally more comfortable sitting forward • Sxs c/w the underlying cause of tamponade • Physical Exam • Beck’s Triad - Elev’d JVP, hypotension, dec’d heart sounds • JVP w/ preserved x descent and dampened or absent y descent • Generally w/ narrow pulse pressure • Tachycardia, other signs of HF (tachypnea, diaphoresis, cool extremities, cyanosis, etc) • Pulsus paradoxus • Dec’d or absent cardiac impulse • +/- Friction rub
Pulsus “Paradoxus” • Dec in SBP > 10-12 mmHg w/ inspiration • Can also occur in pts w/ COPD, pulm dz, PTX, severe asthma • Can have tamponade w/o pulsus paradoxus • In pts w/ pre-existing elev’s in diastolic pressures and/or volume (eg, LV dysfnx, AI and ASD)
Diagnosis • Tamponade is a Clinical Diagnosis • Other Detection Methods • EKG • CXR • TTE • R Heart Cath • CT, MRI
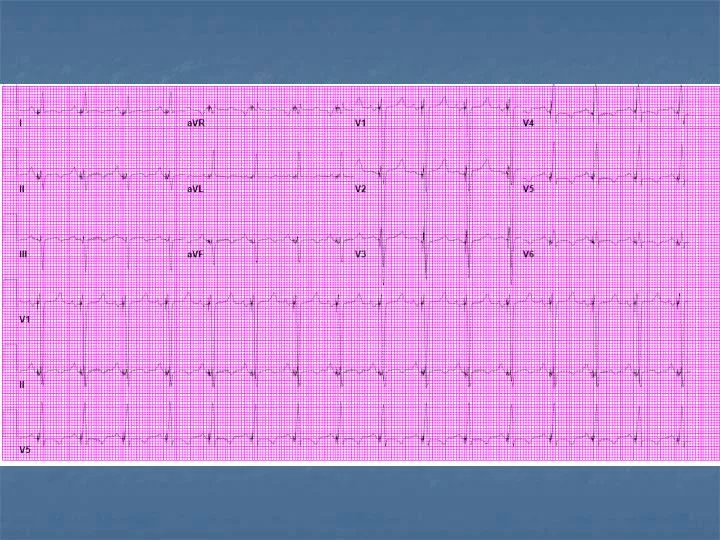
EKG Findings Common Findings Sinus tachycardia Non-specific ST segment and T wave changes Changes assoc’d w/ acute pericarditis (incl diffuse STE & PR depression) Other Findings Dec’d voltage (non-specific and can also be d/t emphysema, infiltrative myocardial dz, PTX, etc) Electrical alternans (specific but relatively insensitive for lg effusions) 2/2 anterior-posterior swinging of the heart w/ each beat Best seen in leads V2 to V4 Combined P wave and QRS complex alternation (specific for cardiac tamponade)
CXR Findings Sudden inc in size of cardiac silhouette w/o specific chamber enlargement Effacement of the normal cardiac borders Development of a “flask” or “H2O-bottle” shaped heart
Lateral CXR Findings May have (+) fat pad sign Separation of mediastinal / retrosternal fat and epicardial fat by > 2 mm
TTE • Test of choice for rapid assessment of pericardial effusions, but these findings are often absent in pts w/ pulm HTN or RVH • Characteristic Findings • Pericardial effusion • Size often correlates w/ risk of tamponade but not always • End-diastolic chamber collapse • RV expiratory collapse in early diastole (low sens, high spec) • RA expiratory collapse in late diastole (high spec if inward movement lasts > 30% of cardiac cycle) • LA collapse (present in ~ 25%, highly spec) • Respiratory variation in transvalvular velocities during passive diastolic filling. • Transmitral resp varn > 25% transtricuspid varn > 50% are char of tamponade. • IVC dilated & fails to collapse w/ inspiration (reflects elev’d CVP) • Small cardiac chambers • Swinging of the heart anteroposteriorly w/in the pericardial effusion • Reciprocal size changes w/ respiration b/w RV & LV & their valves
R Heart Cath Near equalization (w/in 5 mm Hg) of the RA, RV, PCWP, RV diastolic, & LV diastolic pressures RA pressure tracings show diminshed systolic y descent
Tx of Cardiac Tamponade • If mild, can sometimes tx w/ medical mgmt • Including 1 or more of the following: NSAIDs, Colchcine, and/or steroids, depending on the suspected cause. • Require very close monitoring, including w/ serial TTEs and/or RHC
Tx of Cardiac Tamponade • Most require urgent/emergent pericardiocentesis • Closed pericardiocentesis • Generally in cath lab but can be at bedside • Subxiphoid approach under echo guidance is most common - minimizes risk & can assess completeness of fluid removal • Can alternatively use Fluoroscopic guidance • Pigtail catheter often left in place • Open Pericardiocentesis in the OR • May be best for loculated effusions, effusions containing clots or fibrinous material, and/or effusions that are borderline in size • Allow for bx and creation of a pericardial window for recurrent effusions • Bedside pericardiocentesis if pt is in extremis
Emergency Bedside Pericardiocentesis 16- or 18-gauge needle inserted at angle of 30-45° to the skin, near the left xiphocostal angle, aiming toward the L shoulder
Tx of Cardiac Tamponade – Other Measures • IVFs, especially if hypovolemic or if diuretics were given for dx of HF • Temporary inotropic support (Dobutamine, Dopamine) • Serial echos after draining the fluid • Analysis of pericardial fluid • Only has a low yield in determining the etiology of pericardial dz • Can send for specific gravity, pH, glc, LDH, protein, cell count, cytology, staining & Cx for bacteria, fungi, & TB).
Tx of Recurrent Effusions • Pericardectomy • Pericardial-peritoneal shunt • Pericardiodesis - Steroids, tetracycline, or anti-neoplastic drugs administered into the pericardial space sclerosis of the pericardium
References Spodick, DH. Acute cardiac tamponade. N Engl J Med 2003; 349:684. Internet Journal of Anesthesiology 2001: Cardiac Tamponade Secondary To Suppurative Pericarditis. A Case Report And Review Of The Literature Troughton, RW, Asher, CR, Klein, AL. Pericarditis. Lancet 2004; 363:717. Reddy, PS, Curtiss, EI, O'Toole, JD, Shaver, JA. Cardiac tamponade: hemodynamic observations in man. Circulation 1978; 58:265. Roy, CL, et al. Does this patient with a pericardial effusion have cardiac tamponade. NEJM 2007; 297(16):1810-1818 MD Consult Books Libby – Braunwald’s Heart Disease Roberts – Clinical Procedures in Emergency Medicine Adam – Grainger & Allison’s Diagnostic Radiology Goldman - Cecil Medicine LearningRadiology.com