Download
1 / 21
210 likes | 407 Views
Impact of Early Initiation of Combination Antiretroviral Therapy on Measures of Virus in Peripheral Blood of Vertically HIV-1-Infected Children.

E N D
Impact of Early Initiation of Combination Antiretroviral Therapy on Measures of Virus in Peripheral Blood of Vertically HIV-1-Infected Children Jason Brophy1, Tae-WookChun2, Lindy Samson1, Fatima Kakkar3, Hugo Soudeyns3, Mario Ostrowski4, S. Mujib5, John Kim6, Paul Sandstrom6, Richard Harrigan7, Stanley E. Read8, Ari Bitnun8 1. Children’s Hospital of Eastern Ontario, University of Ottawa; 2. National Institute of Allergy & Infectious Diseases, National Institutes of Health, U.S.A.; 3. CHU Sainte-Justine, Université de Montréal; 4. Department of Immunology and Medicine, University of Toronto, 5. University of Toronto, Institute of Medical Sciences, Department of Medicine; 6. National HIV & Retrovirology Laboratories, Public Health Agency of Canada; 7. University of British Columbia, British Columbia Centre for Excellence in HIV/AIDS; 8. Hospital for Sick Children, University of Toronto
Early Combination Antiretroviral Therapy in Infants • The “Mississippi baby” received early cART – experienced a 2-year “viral remission” after stopping treatment until a recent viral rebound • raises the possibility of this as an intervention to limit reservoir establishment and enable “viral remission” • Triple cARTas HIV-post exposure prophylaxis has been routinely administered to newborns at high risk for HIV infection in our centres for many years • SickKids (Toronto), CHEO (Ottawa), and CHU Ste-Justine (Montreal)
Objectives • To investigate HIV-1 reservoirs in peripheral blood of HIV-1-infected children with SVS following initiation of cART within 72 hours of birth • SVS: defined as absence of detectable virus in standard viral load (VL) assay subsequent to having achieved an undetectable VL (< 50 copies/mL)
Methods • Retrospective review at our 3 centres of all children born to HIV-infected mothers who received triple cART within 72 hours of birth • Evaluation of HIV reservoir, immune responses, and genetic characteristics in those infected children with SVS after cART
Results – Retrospective Review • 136 infants received triple cART • HIV infection in 12 (8.8%) • In utero infection probable in at least 50% (n=6; HIV PCR positive within 48 hours of birth) • Timing uncertain in 50% (n=6) as testing done after 48 hrs • Four HIV-infected children achieved SVS (Cases 1-4) • Eight HIV-infected children did not achieve SVS • 6 of 8 did not achieve virologicsuppression due to poor adherence • 2 of 8 initially suppressed for 2-3 years, then experienced viral rebound after poor adherence (one during the course of our study – Case 5)
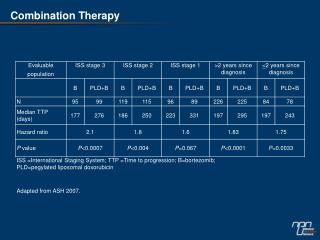
Reservoir Evaluation of 4 Early-Treated, HIV-Infected Children • Cases 1 to 4 had SVS from 2-7 years • All 4 remained on their original cART regimen of zidovudine, lamivudine, and nevirapine
Maternal Characteristics and Infant Diagnostic Testing * Non-identical twins; ** mother died soon after delivery from OI
Case 1 • Now 7.5 years old • Remains on same ART combination • Has maintained an undetectable • viral load CD4 count 3940 (55%) cART initiated (day 1) HIV DNA PCR positive (day 1)
Case 2 • Now 7.5 years old • Remains on same ART combination • Undetectable viral load CD4 count 1447 cells/L (28.9%; day 20) cART initiated (day 1) HIV DNA PCR positive (day 2)
Cases 3 & 4 CD4 count 1997 cells/L (41%, day 17) CD4 count 2663 cells/L (63%, day 15) 795 c/mL (day 12) cART initiated (day 1) HIV DNA PCR positive (day 1) cART initiated (day 1) HIV DNA PCR positive (day 1) • Now 3 years old • Remain on same ART combination and have sustained virologicsuppresSion
‡ Limit of detection: 1.5 copies/mL; each assay performed on 6 mL of whole blood; § Limit of detection: 1.5 g RNA; performed in duplicate; ¶ Limit of detection; 20 copies/ml; ¥ HLA-B variation at positions associated with better virologic control (lower set-point) and specific protective amino acid substitutions are indicated in bold
Case 5 CD4 2568 (46.2%) CD4 2299 (37.3%) CD4 2145 (40.0%) CD4 2584 (39.3%) CD4 1995 (38.3%) HIV DNA PCR positive (Day 4) cARTchanged (day 21) - AZT/3TC/LPV cART started (day 1) - AZT/3TC/NVP
Discussion • Absence of detectable HIV DNA and absent/very low levels of replication-competent virus in peripheral blood and lack of HIV-specific immune responses demonstrated in a subgroup of children initiated on cART<72 hours of birth • Suggests early cART initiation can greatly reduce HIV reservoir size • Genetic factors may also play an important role - protective HLA genotypes were found in 3 of 4 children • HLA B*58 • Sequence variation at HLA-B positions 67, 70 and 97 (associated with superior control of HIV replication) • The child with replication competent virus did not have these protective genotypic features International HIV Controllers Study, Science 2010 Lazaryan, J Virology 2006; Lazaryan, J Virology 2010
Discussion • Our 5th case with rapid viral rebound after interruption of therapy despite limited reservoir size demonstrates that early cART will not be effective in all patients • Multiple factors may have influenced this patient’s outcome • Baseline NNRTI resistance, sub-optimal initial regimen • Low-level detectable VL after initial suppression • This, along with late relapse of viral replication in Mississippi baby, underscore the need for better understanding of contributing factors to reservoir & viral control • Host and viral genetics • Timing and completeness of initial viral suppression • Selection of components of cART regimen in infants
Conclusions • Based on our study findings and other reports, early cART for HIV-infected infants clearly limits size of viral reservoir • Additional non-blood reservoir sites require investigation • The clinical significance and benefit of this remain to be seen • Accurate estimation of size of HIV viral reservoir in children is significantly impacted by limitations in collection of adequate blood volumes in children compared with adults • A prospective multi-centreobservational study (EPIC4) is underway in Canada to determine the impact of early versus later treatment on reservoir size and HIV control in children
Acknowledgments • The children and parents who agreed to participate in this study • The Canadian Institutes for Health Research, Canadian Association for AIDS Research, and the International AIDS Society for funding to carry out EPIC4 study
Reservoir, Immunologic Responses and Genetics • Level of cell-associated HIV-1 DNA in CD4+ Tcells • real-time PCR • Levelofcell-associated HIV RNA • CobasAmpliprep/CobasTaqman HIV‐1 assay • Residual plasma viremia • modified CobasAmpliprep/CobasTaqman HIV‐1 assay • Presenceofreplicationcompetentvirus • levelofvirion-associated HIV RNA in culturesupernatantaftermitogenicstimulation • co-cultureassay • HIV serology; HIV-specific cell-mediated immune responses; HLA typing and CCR5 delta 32 genotyping
‡ Limit of detection: 1.5 copies/mL; each assay performed on 6 mL of whole blood; § Limit of detection: 1.5 g RNA; performed in duplicate; ¶ Limit of detection; 20 copies/ml; ¥ HLA-B variation at positions associated with better virologic control (lower set-point) and specific protective amino acid substitutions are indicated in bold