Download
1 / 44
450 likes | 805 Views
A Case of Cauliflower Ears. Hilary Rowe, BScPharm VIHA Pharmacy Resident 2009-10 Pain Clinic Rotation. Outline. Objectives Background Patient Case Clinical Question Review of Evidence Recommendation Monitoring. Objectives.

E N D
A Case of Cauliflower Ears Hilary Rowe, BScPharm VIHA Pharmacy Resident 2009-10 Pain Clinic Rotation
Outline • Objectives • Background • Patient Case • Clinical Question • Review of Evidence • Recommendation • Monitoring
Objectives • Describe 1 way inflammation destroys cartilage in relapsing polychondritis (RP) • Name 3 risk factors for addiction in a pain patient • Be familiar with the evidence of disease modifying agents in RP
Relapsing Polychondritis • Destruction of cartilage and replacement with fibrous tissue • Autoantibodies to type II, IX, XI collagen causes inflammatory infiltration • Produce Th1 cytokines (TNF-α) by T-cell clones reactive to Type II collagen • Lysosomal enzyme release eventually results in destruction of the cartilage
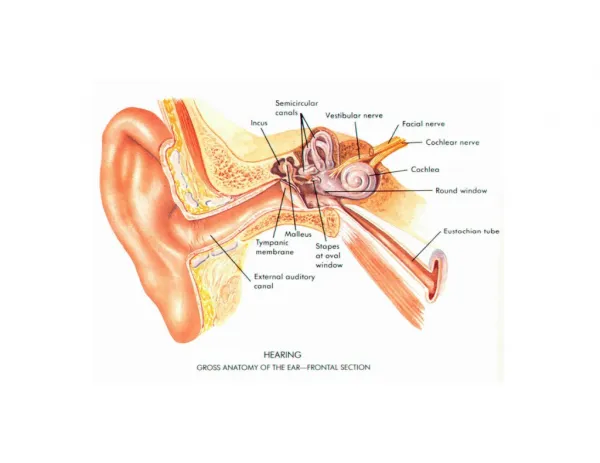
Diagnostic Criteria Presence of 3 or more: • Recurrent chondritis both auricles • Non-erosive inflammatory polyarthritis • Nasal chondritis • Ocular inflammation • Respiratory tract chondritis • Cochlear &/or vestibular dysfunction
Treatment ? Methotrexate, Colchicine, Dapsone, Hydroxychloroquine Treat inflammation-Prednisone Treat pain-NSAIDS Diagnosis
Mrs. MJ • ID: 40 yo female, ht 155cm, wt 62kg • CC: Acute decline in functioning with widespread pain and stiffness in joints • HPI Nov 2009:Current RP flare of longest duration; walking this summer and now in motorized wheel chair since September • RP diagnosed Aug 2009, polyarthritis since 2005
Mrs. MJ • PMHx:Transposition of ureters 1983- Recurrent UTI’s (prior to surgery 8-9/year, after surgery 1-2/year) • Allergies: Lactose (hives & difficulty breathing)
Mrs. MJ • Social & Family Hx: • Lives with husband & two teenagers • Prior to attack was running an event planning business • Both parents were alcoholics • Discharge Plan from Pain Clinic: • Improve pain control & function
Medical Problem List Active: • Prolonged flare of RP • Pain • Constipation Chronic: • Depression • Osteopenia • RP • Graves disease • Pain
Score is 5: • 3 points family history • 1 point age • 1 point depression • Other factors: • Drug seeking • Altering routes • Running out early • Rx forgery • Stealing • ↑ dose with no change in disease state
Pain History Paroxysmal attacks: • Left side more affected then right • Described: red-hot poker stabbing and digging into her • 20/10 causing her to sob, occurs with flares • What makes it better-? more medication • What makes it worse- Nothing
Pain History Baseline aches: • Widespread: Nose, chest, sternum, jaw, elbows, back, shoulders, wrists, hands, hips, ankles • Described: ache • What makes it better-baths, medication • What makes it worse- > 300-400 steps per a day
DRPs • MJ has a prolonged polychondritis flare and is experiencing additional pain not controlled by her current therapies • MJ is experiencing constipation secondary to narcotics and immobility and could benefit from a regular bowel routine
DRPs • MJ has a prolonged flare of polychondritis and could potentially benefit from re-evaluation of her disease modifying agents
Question • Are there any disease-modifying therapies that might be helpful for Mrs. MJ’s prolonged flare of relapsing polychondritis, taking into consideration the medications she has already tried?
Therapeutic Options • No change in therapy • Infliximab • Rituximab • Azathioprine • Cyclophosphamide
Search Strategy • PubMed, Embase, Google • Search terms: • Relapsing polychondritis • Disease modifying agents • Autoimmune diseases • Found • 3 case reports, 1 retrospective review
Leroux et al. Arthritis & Rheumatism 2009 • Results: • 2 partial remissions • 4 stable • 3 worsened • 2 added new immunosuppressants • 2 increased steroid dose • 6 benefitted- at 12 months 2 remained stable & 4 were worse
Goals of Therapy Patients Goals • Improve pain control • Increase mobility and ADL • Return to work Team Goals • Improve pain control • Increase mobility and ADL • Slow progression of disease • Decrease morbidity & mortality • Minimize adverse drug events
Recommendation • No definitive evidence to support suggesting a disease-modifying agent • Risks and benefits of infliximab should be discussed with patient • Patient should make an informed decision to start therapy
Recommendation • Improve pain control • Discontinue Codeine Contin • Start Morphine 30mg long acting q 12h • Start Morphine IR 5mg prn for breakthrough pain
Recommendation • Codeine Contin ineffective pain 20/10, poor sleep, dose above ceiling effect of 400mg/day • Morphine is effective for breakthrough pain • Morphine less potential for abuse then hydromorphone and oxycodone • SR formulation less potential for abuse
Follow Up- Feb 2010 • Patient switched from Codeine Contin to Morphine (↓ IR 2 daily to 2-3 nights/wk) • Currently ↓ prednisone dose • Patient wanted to trial dapsone & colchicine 1st (DMARD was not started) • Patient now considering DMARD option • Constipation improving
References • Kahan M, Srivastava A, Wilson L et al. Misuse of and dependence on opioids: study of chronic pain patients. Canadian Family Physician 2006;52:1081-87. • Marie I, Lahaxe L, Josse S, Levesque H. Sustained response to infliximab in a patient with relapsing polychondritis with aortic involvement. Rheumatology 2009 Oct;48(10):1328-33. • Leroux G, Costedoat-Chalumeau N, Brihaye B, et al. Treatment of relapsing polychondritis with rituximab: a retrospective study of nine patients. Arthritis Rheumatology 2009 May 15;61(5):577-82. • Buonuomo PS, Bracaglia C, Campana A, et al. Relapsing polychondritis: new therapeutic strategies with biological agents. Rheumatology International. 2009 Aug 15. [Epub ahead of print]. • RichezC, Dumoulin X, Schaeverbeke T. Successful treatment of relapsing polychondritis with infliximab. Clinical and Experimental Rheumatology 2004;22:629-31. • PorroGB, Lazzaroni M, Imbesi V et al. Efficacy of pantoprazole in the prevention of peptic ulcers, induced by non-steroidal anti-inflammatory drugs: a prospective, placebo-controlled, double-blind, parallel-group study. Digestive and Liver Disease 2000 April; 32(3): 201-208.