Download
1 / 62
620 likes | 830 Views
ANEMIAS Nazzal Bsoul,MD Al Bashir Hospital. DEFINITION. Anemia : Is defined as a reduction in one or more of major RBC measurements. Hemoglobin ( Hb ). Hematocrit (HTC). Red blood cells count (RBCs) . Anemia is not a disease by itself but is one of the major signs of disease.

E N D
ANEMIAS NazzalBsoul,MD Al Bashir Hospital
DEFINITION Anemia: Is defined as a reduction in one or more of major RBC measurements. Hemoglobin (Hb). Hematocrit (HTC). Red blood cells count (RBCs) . Anemia is not a disease by itself but is one of the major signs of disease. May be the first manifestation of a systemic disease,along with other nonspecific complaints such as fever,weightloss,anorexia.
HEMOGLOBIN (Hb) Hb Concentration: measures the major oxygen-carrying pigment in whole blood. Values are expressed as grams of Hb per dL of whole blood (g/dL). Normal range: M 13-16,5 g/dL F 12-15,5 g/dL
HEMATOCRIT Hematocrit (HTC): Is the percent of a volume of whole blood occupied by intact RBCs. Values are expressed as a percentage. Normal range: M 41-51%. F 37-47%.
RED BLOOD CELL COUNT (RBCs) RBC Count: Is the number of RBCs contained in a unit of whole blood. Values are expressed as millions of cells per uL of whole blood. Normal range: M 4,5-6,5 millions/uL F 3,8-5,8 millions/uL
VOLUME STATUS The three measurements are all concentrations. As such they are dependent upon both the RBC mass and the plasma volume. 1.In acute bleeding, anemia develops only after 36-48 hours. 2.Pregnancy: RBC mass is increased by 25% and plasma is increased by 50%.Normal values in pregnancy are diffirent. 3. Dehydration.
SPECIAL POPULATIONS 1.Living at high altutute. 2.Smoking and air pollution. 3.African-Americans—lower values. 4.Populations with a high incidence of ch.diseases. 5.Athletes. 6.The elderly:should not have a lower normal range for fear of missing a serious underlying disorder.
ERYTHROPOESIS -1 Erythropoesis takes place in adults within the BM under the influence of the stromal framework,a number of cytokines,and the eryrhroid specific growth factor,erythropoietin(EPO). EPO is a true endocrine hormone produced in the kidney. EPO enhances the growth and differentiation of the 2 erythroid progenitors. 1.Burst Forming Units-erythroid/BFU-E/. 2.Colony Forming Units-erythroid/CFU-E/.
ERYTHROPOESIS-2 • The rate of RBC production equals the rate of RBC destruction. • Approximately 1% of RBCs is removed from the circulation daily. • The rate of RBC production can be increased markedly (5-7 folds).
CLINICAL CONSEQUENCES OF ANEMIA The signs and symptoms induced by anemia are dependent upon the degree of anemia as well as the rate at which the anemiahas evolved. Symptoms of anemia can result from two factors: 1.Decreased O2 delivery to tissues. 2.Hypovolemia (acute bl.loss).
COMPENSATORYMECHANISMS Signs and symptoms depend also on the compensatory mechanisms. 1.Extraction of O2 by the tissues can increase from 25% to 60%. 2.Cardiac compensation: stroke volume and heart rate (cardiac output). Thus normal O2 delivery can be maintained by 1and 2 at rest at HBG as low as 5g/dL,assuming that the intravasc.volume is maintained. Thus symptoms will develop when HBG falls below this level at rest or at higher HBG during exersion or when cardiac compensation is impaired.
SYMPTOMS AND SIGNS Symptom:is a sensation or change in health function experienced by the patient. It is a subjective report. Fatigue/tiredness Pain. Nausea. Dizziness.
SYMPTOMS AND SIGNS-cont’d Sign: is an objective evidence of the presence of a disease or disorder. Signs are discovered and reported by the physician,not by the patient.It is an objective report. Elevated BP. Skin rash. Tachypnea. Tachycardia.
SYMPTOMS AND SIGNS OF ANEMIA Dyspnea/S.O.B.:on exersion/at rest. Fatigue/tiredness. Signs and symptoms of hyperkinetic state: 1.bounding pulses. 2.palpitations. 3.roaring in ears. In more severe anemia:Lethargy,confusion,CHF,angina,MI. Pallor. Headache. Complications of extracellular volume depletion (in acute bleeding).
CAUSES OF ANEMIA There are 2 interrelated approaches one can use to help identify the cause of anemia. 1.Kinetic approach. 2.Morphologic approach.
KINETIC APPROACH Anemia can be caused by one or more of 3 independent mechanisms. 1.Decreased RBC production. 2.Increased RBC destruction. 3.RBC loss.
Decreased RBC PRODUCTION • If less than 1% of the circulating RBCs is replaced by the BM. 1- Lack of nutrients such as iron,B12,or folate. 2- Primary involvement of the BM such as aplastic anemia,PRCA,MDS,or tumor infiltration. 3- Low levels of trophic hormones,such as EPO in CRF,thyroid hormones,and androgens.
INCREASED RBC DESTRUCTION • A RBC life span below 100 days is the operational definition of hemolysis. • Anemia will ensue when the BM is unable to keep up with the need to replace more than 5% of the RBC mass daily. 1-Inherited hemolytic anemias: hereditary spherocytosis,SCD,and thalassemia major. 2-Aquired hemolytic anemias: AIHA,TTP.
RBC LOSS • Blood loss is the most common cause of anemia • Forms of bleeding: 1-Obvious bleeding: trauma,melena, hematemesis,ormenometrorrhagia. 2-Occult bleeding:a slowly bleeding colonic polyp or carcinoma. 3-Iatrogenic bleeding: Excessive bl. donations,or repeated venesection.
MORPHOLOGIC APPROACH According to RBC size. Mean Corpuscular (Cell) Volume (MCV). RBC size (MCV) is 80-96 femtoliters(fL). Microcyte. Macrocyte. Normocyte.
ANEMIAS ACCORDING TO THE RBC SIZE 1.Microcytic anemia. 2.Macrocytic anemia. 3.Normocytic anemia.
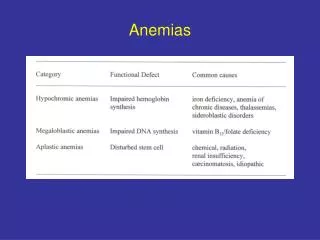
MICROCYTIC ANEMIAS Are associated with an MCV below 80 fL. 1-Iron Deficiency Anemia (IDA) 2- Anemia of Chronic Disease (ACD) 3-Thalassemias.
IDA,ACD,and thalassemias are the most 3 common causes of microcytosis in clinical practice. • Since all 3 have hypochromic and micro- cytic RBCs on blood film (smear),other factors must be used to establish the diagnosis.
IRON DEFICIENCY ANEMIA (IDA) • Important discriminating features are: 1-Low serum iron concentration. 2-Increased total iron binding capacity (TIBC) 3-Low serum ferritin concentration. 4-High RDW. • It is mandatory to determine the cause of iron deficiency.
ANEMIA OF CHRONIC DISEASE (ACD) • The hallmarks of this condition are: 1-Low serum iron. 2-Low TIBC. 3-Normal to increased serum ferritin concentration. • The causes are usually related to the presence of chr.infection (TB), inflamation (RA),or malignancy.
ALPHA OR BETA THALASSEMIA MINOR • Adults with thalassemia are most often heterozygotes for the alpha or beta forms of this syndrome,and may not be anemic. • Family history is often negative. • P/E may reveal splenomegaly. • Blood film: microcytosis,hypochromia, target cells,tear-drop forms,and basophilic stippling.
MACROCYTIC ANEMIAS Are characterized by an MCV above 100 fL. Reticulocytosis. Vit.B12 def. Folate def. MDS. Hypothyroidism
NORMOCYTIC ANEMIAS By definition the MCV is normal. ACD. MDS.
MULTIPLE CAUSES OF ANEMIA • In pediatric practice anemia is commonly caused by a single disorder. • In adults,mainly older adults,multiple causes are frequently present. 1-Ca colon: IDA and ACD 2-AIHA on steroids and GI bleeding. 3-RA and NSAIDs: ACD and IDA
EVALUATION OF THE PATIENTWITH ANEMIA-1 • Anemia is one of the major signs of disease. • It is never normal and it`s cause should be always be sought. • History. • Physical examination. • Simple lab.tests. • Other investigations.
EVALUATION OF THE ANEMIC PATIENT-2 The workup should be directed towards answering the following questions: 1.Is the patient bleeding (now or in the past) ? 2.Is there evidence of increased RBC destruction? 3.Is the BM suppressed?. 4.Is the patient iron deficient? if so,why?.
HISTORY • Symptoms related to anemia (melena,CRF,RA) • Etnicity and country of origin (Hemoglobinopathies). • Drug history (NSAIDS).
PHYSICAL EXAMINATION • Pallor. • Jaundice. • Tachycardia. • Lymphadenopathy. • Hepatosplenomegaly. • Bone tenderness.
LABORATORY EVALUATION-1 • Complete blood count (CBC): HBG,HCT, RBC count,RBC indices,and WBC count. • WBC differential,PLT count,and reticulocyte count. • Blood film (Blood smear). • Red cell distribution width.
LABORATORY EVALUATION-2 Red cell indices: 1-Mean corpuscular volume.MCV 80-100 femtoliter. 2-Mean corpuscular hemoglobin.MCH 27,5-33,2 picograms of hemoglobin per RBC. 3-Mean corpuscular hemoglobin concentration.MCHC.33,4-35,5 grams of hemoglobin per dL of RBCs.
Red Cell Distribution Width(RDW) • RDW is a measure of anisocytosis or variation in red cell size. • Increased RDW is commonly found when there is a nutritional deficiency(eg,iron ,folate,and Vit.B12). • Increased RDW is not specific for any one abnormality. • An increased RDW is the mathematical equi- valent of the term”anisocytosis”,but is not diagnostic of any particular morphologic finding.
LABORATORY EVALUATION-3 • Reticulocyte count: helps to distinguish among the different types of anemia. 0,5-1,5 percent. Absolute reticulocyte count.25,000- 75,000/uL. Reticulocytes normally survive for 4 days,of which 3 days in the BM and one day in the peripheral circulation. • White blood cell count (WBC count). • Neutrophil hypersegmentation. • Platelet count (PLT count).
OTHER INVESTIGATIONS • Bone marrow aspirate and trephine biopsy. • Radiological studies. • Genetic studies. • Immunological studies.
BONE MARROW EXAMINATION • BM examination generally offers little additional diagnostic information in the more common forms of anemia. • Although the absence of stainable iron in BM is considered the “gold standard” for the diagnosis of ID,this diagnosis is usually established by lab.tests alone.
BONE MARROW EXAMINATION-Cont’d • Indications for BM examination in anemic patients include: 1-Pancytopenia. 2-The presence of abnormal cells in the circulation (blast forms).
EVALUATION FOR ID • History: menometrorrhagia,symptoms of PUD. • Preliminary lab.data: Low MCV,low MCH, high RDW,high PLT count. • More complete evaluation is needed: Serum iron TIBC serum ferritin
Clinical Manifestations of Iron Deficiency (ID)-1 • The presenting symptoms of ID are caused primarily by anemia: • Weakness,headache,irritability,fatigue, exercise intolerance. • Koilonychia (Spoon nails),blue sclerae, glossal pain. • Cognitive functions-verbal learning, memory,and concentration.
Clinical Manifestations of ID-2 • Physical performance- ID impairs exercise capacity and causes easy fatiguability • PICA and Pagophagia: • PICA:is a perverted apetite for substances not fit as food,such as clay or paper products. • Pagophagia: is PICA for ice.
Causes of ID • Blood loss:Commoncause.Overt or occult. • Decreased iron absorption: Relatively uncommon cause. • Intravascular hemolysis: Hematuria (PNH). • Pulmonary hemosiderosis: • Administration of erythropoietin: In anemia of chronic renal failure.
Diagnosis of ID-1 • History and physical examination. • Laboratory investigations: CBC,RBC indices,and blood film(smear)→pre- sumptive diagnosis of ID. • Therapeutic trial of oral iron→positive response (reticulocytosis,followed by an increase in Hb at a rate of about 2-4 g/dL every 3 weeks
Diagnosis of ID-2 • No positive response ? • The following lab.investigations are needed at the beginning: 1-Serum Iron (SI) 2-Total Iron Binding Capacity (TIBC) 3-Transferrin Saturation: (SI ÷TIBC)% 4-Serum ferritinlevel.
Search for Source of Bleeding and Iron Loss • Diagnosing the cause of ID is much more important than diagnosing ID. • History and physical examination. • Other investigations: Upper and lower endoscopy.
Classic Presentation of IDA • A multigravid woman in her 40’s,presents with tirednes and fatigue and chronic blood loss from menometrorrhagia.The following lab. findings were noted: 1-The hemoglobin was 8 g/dl,with MCV of 75 fL. 2-The MCH and MCHC were both low. 3- Blood film showed microcytic,hypochromic red blood cells(RBCs) 4-The serum iron was low and the total iron binding capacity(TIBC) was elevated,resulting in transferrin saturation < 15%.The plasma ferritin concentration was reduced.
Classic presentation of IDA-Cont’d • Iron stores were absent after performing the “gold strandard” test for estimating iron stores via bone marrow aspirate of the patient. • Finally,the patient responded briskly to oral iron therapy with a reticulocytosis followed by elevations in the hemo- globin concentration.
VITAMIN B12 AND FOLATE DEFICIENCY ANEMIAS Dr.NazzalBsoul