Download
1 / 63
630 likes | 644 Views
Learn about the benefits of the banded gastric bypass procedure for long-term weight loss and maintenance. Explore the evidence and success rates of this surgical treatment option.

E N D
Who Would Have Thought It? Banded Gastric Bypass Works! MAL Fobi MD FACS, FICS, FACN Medical Director Center for Surgical Treatment of Obesity Long Beach CA, USA
Banded Gastric Bypass Disclosures President of Bariatec Corporation. A device Compny I had a Banded Gastric Bypass
Why the Banded Gastric Bypass? Obesity, particularly Morbid Obesity, is a life long disease that is recalcitrant to any treatment, even surgical treatment.
Obesity is a disease with a Genetic Predisposition PSYCHO- LOGICAL DIS. The exact method of genetic translation is not known at this time. The Expression of obesity varies with social, cultural, environmental, economic and psychological influences. SOCIO-ECOMOMICS EATING DIS. HORMONAL IMBALANCE WILL POWER GENETIC
Significant ramifications of obesity MEDICAL PSYCHOLOGICAL ECONOMIC SOCIAL
NIH Consensus Statements 1991 • Prolonged and sustained weight loss has not bee proven with drug therapy. • * • Published studies of medical approaches to treatment of obesityinclude few reports or indications of efficacy in person with clinically severe obesity. • * • Evidence of long-term efficacy of behavior modification in persons with clinically severe obesity is lacking. • * • VLDC's used under close medical supervision generally have not been successful for achieving permanent weight loss.
Surgical Treatment and Management of Obesity Surgical Treatment is the only treatment that provides effective long-term control Gastric Bypass/Banded Gastric bypass Gastroplasty/Sleeve Gastrectomy Gastric Banding Bilio-pancreatic Diversion with or without a Switch Intestinal Bypass
Mason Gastroplasty 1971 • Simple operation??? • As effective • Less morbidity • Less mortality
Evolution of the Gastric Bypass Linner’s Banded Gastric Bypass 1984
Evolution of the Gastric Bypass Salmon’s Banded Vertical Gastroplasty Distal RYGBP 1986
Evolution of the Gastric Bypass Banded Gastric Bypass Fobi Modification 1986
VBG VS. GBP 3-4cm VS Howard, Obesity Surgery, 1995
VBG VS. GBP Howard, Obesity Surgery, 1995
Average PEWL (All Pts.) Banded Gastric Bypass Fobi Obes. Surg. 2005
Why the Banded Gastric Bypass • Historical and Experimental Data: • There are eight series with long term (6-14years) follow-up documenting 70+ PEWL and weight loss maintenance in more patients, even the old and super obese • Capella, USA, AJS; Fobi, USA, SOARD; White, New Zealand, ObesSurg; Salinas, VenuzuelaSOARD; D.Margo, ObesSurg; Mali, ObesSurg; Cruz, ObesSurg; and Awad, Obesity Surgery 2012 • There are only six long term series reported with the non-banded gastric bypass with an average of 55 PEWL, except Sutter with 70+ PEWL • Pories, Sutter, Dinitz, Christou, Higa, and the Swedish study
Banded vs Non Banded Gastric Bypass % EWL Awad et al Obes. Surg. 2012 83,5(45-115) 61,5(27-109) There is a significative difference in %EWL at 36-96 month. We followed the banded patients for 10 and 12 years and they maintained the same %EWL. Presented at IFSO_LAC Congress Cartagenia, Columbia, March 2011
Banded Gastric Bypass vs. Non-Banded Gastric Bypass Dr. Lemmens IFSO Dehli 2012 Retrospective Review
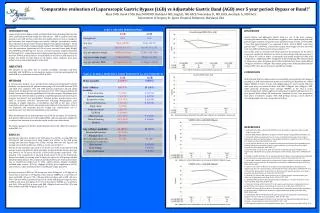
Prospective comparative evaluation of the Laparoscopically banded gastric bypass vs. the Laparoscopically non-banded gastric bypass. Banded GBP Non-Banded GBP (n=20) (n=20) BMI 58.7 51.18 Age (years) 46 47 6 months %EWL 43.1 38.6 12 months %EWL 64.0 57.800 36 months %EWL 67.6 55.7 Complications %(n) 20%(5) 35%.(7) % of patients achieving 50%EWL 85% 65% BGBP vs. GBP Fobi et al IFSO 2011 Hamburg Germany
Prospective comparative evaluation of the Laparoscopically banded gastric bypass vs. the Laparoscopically non-banded gastric bypass in the super obese. Banded GBP Non-Banded GBP (n=46) (n=44) BMI 59.4 59.7 Age (years) 40.6 42.6 6 months %EWL 43.1 24.7 12 months %EWL 64.0 57.8 24 months %EWL 64.2 57.1 38 months %EWL 73.4 57.7 Complications %(n) 23.9 (11) 29.5 (13) % of patients achieving 50%EWL 63% 45% His conclusion: It appears the banded gastric bypass produces more weight loss in more patients Banded Gastric Bypass VS. Non Banded Gastric Bypass. Marc Bressler, SOARD, July/August 2007
BGBP vs. GBP Schauer and Associates at the Cleveland Clinic • Presented Prospective Evaluation with two year follow-up at IFSO Congress in Hamburg (2011) • Showed more weight loss and maintenance with the BGBP
Banded Gastric Bypass vs. Non-Banded Gastric Bypass Karcz et al. GaBP Ring European multicenter clinical trials. IFSO, Dehli 2012
BGBP vs. GBP Herrera, Mexico, SOARD 2009 • Prospective Evaluation with two years follow-up • Showed no difference
Banded Gastric Bypass Published reports of band placement in failed gastric bypass document increased weight loss and waight loss maintenance • Bressler M. Obes Surg 2005;15:1443-48 • Kyzer S. Obes Surg 2001;11:66-9 • Gobble RM. Surg Edosc. 2008;22:1019-22 • Heath D. Obes Surg 2009;19:1439-41 • Himpens Obes Surg 2001, 11(4):528-31 • Avinoah E. obes surg 2006; 6:213-15
Adjustable Band Placement for Revision of failed Gastric Bypass Bressler Obes. Surg. 2005
Banding the Pouch in GBP “Since Roux-en-Y Gastric Bypass is primarily a restriction operation, just as with VBG, it is important that the outlet of the pouch does not stretch.” ( E.Mason,Obesity Surgery 1994; 4:66-72)
Banded Gastric Bypass At this time, the most promising technique based on a large series is that described by Capella and Capella, the “Banded Gastric Bypass” MacLean, J Am CollSurg 97; 185:1-7
Why the Band in the Gastric Bypass Operation • Fisher after an in depth review concluded that “Long-term results suggest that a silastic ring encircling the stomach pouch proximal to the gastroenterostomy may improve the outcome following gastric bypass surgery, resulting in more weight loss by a greater number of patients sustained for a longer time” - Fisher BL, Barber AE, Eur J Gatroenterol Hepatol 1999; 11:93-97
%EWL for standard RYGBP and its two hybrid forms of LL-RYGBP and Banded RYGBP (* P < 0.05). [O’Brien P.E.:Systemic review of mdium term-weight loss after bariatric surgery.; Obesity Surgery:2006; 16; 1032-40]
Banded Gastric Bypass • Why and how does banding the pouch make it more effective for weight loss and Weight loss maintenance? - Fobi, www.bariatec.com
Non-banded Roux-en-Y GBP Reservoir size change with time
Banded Roux-en-Y GBP Reservoir size change with time
Ring Banded Gastric Bypass Stubbs, Obes Surg; 2005
3-D Recon Image of Ring Banded Gastric Bypass French Catheter Size 1 Fr. = 1/3 mm diameter 34 Fr. = 1.13cm diameter 40 Fr. = 1.33cm diameter 60 Fr. = 2.0cm diameter Ring or band should be loose around the pouch at time of banding Optimal Ring Size 6.5 cm 2.07cm Diameter 1.47cm functional diameter. Mohit Bhandari Indore, India 2012
Banded Gastric Bypass Complications from Banding the Gastric Bypass Band erosion: - 0-7%. Incident directly related to type of the device used, the diameter and size of the device and the presence of contamination or infection. Ring sizes < 6.5cm cause more erosion and dysphagia without increase in effectiveness. Kinking or Slippage: - - 0-1%. Functional Obstruction Treated by endoscopic dilatation or laparoscopic re exploration Solid Food intolerance: - 5-7 %. Not disabling. Treated by dietary counseling. Occasional need for Ring removal
Surgeons have used various devices to band the pouch Surgeon fashioned devices Marlex Mesh Silastic Tubing Ethibond Suture Linea Alba Fascia Porchine Graft Bovine Graft Commercially prefabricated devices GaBP Ring. (Designed for use with the gastric bypass and sleeve gastrectomy) IOC Band AMI Band Minimizer Band Bioring
GaBPRingTM Device GaBP Ring Autolock™ and Gastrostomy Site Marker Clinical Research Study Protocol IDE G050231 IPERSONNEL ---------------------------------------------------------------------------------------------------------2IISTUDY SYNOPSIS --------------------------------------------------------------------------------------------------3IIICLINICAL TRIAL --------------------------------------------------------------------------------------------------51.Introduction and Rationale -----------------------------------------------------------------------------------52.Study Objective ------------------------------------------------------------------------------------------------62.1Effectiveness Endpoints -----------------------------------------------------------------------------62.2Safety Endpoints --------------------------------------------------------------------------------------63.Study Design --------------------------------------------------------------------------------------------------74.Patient Population ---------------------------------------------------------------------------------------------84.1Exclusion Criteria -------------------------------------------------------------------------------------84.2Inclusion Criteria --------------------------------------------------------------------------------------95.Device Characterization -------------------------------------------------------------------------------------95.1Intended Use and Description ------------------------------------------------------------------------96.Study Methods -------------------------------------------------------------------------------------------------106.1Patient Entry and Pre-operative Evaluation -------------------------------------------------------106.2Device Installation and Intra-operative Evaluation -----------------------------------------------116.3Post-operative Care -----------------------------------------------------------------------------------116.4Post-operative Evaluation ----------------------------------------------------------------------------117.Study Procedures ----------------------------------------------------------------------------------------------138.Data Monitoring -----------------------------------------------------------------------------------------------138.1Data Reporting and Monitoring Procedures -------------------------------------------------------138.2Adverse Reaction and Adverse Event Reporting -------------------------------------------------159.Study Analysis -------------------------------------------------------------------------------------------------159.1Sample Sizes -------------------------------------------------------------------------------------------159.2Statistical Methods ------------------------------------------------------------------------------------1510.Bibliography --------------------------------------------------------------------------------------------------16IVAPPENDICES -------------------------------------------------------------------------------------------------------17Appendix 1:Consent to Act as a Human Research Subject -------------------------------------------------17Appendix 2:Device Design and Labeling --------------------------------------------------------------------27Appendix 3:Prior Clinical Investigations --------------------------------------------------------------------44Appendix 4:Surgical Procedure ------------------------------------------------------------------------------50Appendix 5:Device Removal Indications and Procedures --------------------------------------------------57Appendix 6:Examination Procedures, Study Equipment and Techniques -------------------------------58Appendix 7:Sponsor’s Commitments -------------------------------------------------------------------------60Appendix 8:Investigator’s Qualifications and Responsibilities -------------------------------------------61Appendix 9:Investigator’s Agreement ------------------------------------------------------------------------62Appendix 10:Investigator’s Financial Disclosure Declaration ---------------------------------------------65Appendix 11:Declaration of Helsinki/Protection of Human Subjects/Belmont Report/Institutional Review Board --------------------------------------------------------------------------------------66Appendix 12: Physician Information Letter --------------------------------------------------------------------96Appendix 13:Case Report Forms -------------------------------------------------------------------------------105
GaBPRingTM Device GaBP Ring™ is a prefabricated, sterilized ring designed to band the proximal pouch of the sleeve gastrectomy and gastric bypass operations.
Incidence of Band Erosion (May 1992 – May 2002) Banded Gastric Bypass 3,632 (100 %) Primary 3007 ( 82.79 %) Secondary 405 ( 11.15 %) Revision 220 ( 6.06 %) Band Erosion 57 ( 1.89 %) Band Erosion 24 ( 5.92 %) Band Erosion 10 ( 4.54%) Total Incidence of Band Erosion: 91/ 3,632 (2.5 %)
Banded Gastric Bypass vs. Non-Banded Gastric Bypass Dr. Lemmens IFSO Dehli 2012 Retrospective Review