Download
1 / 51
520 likes | 782 Views
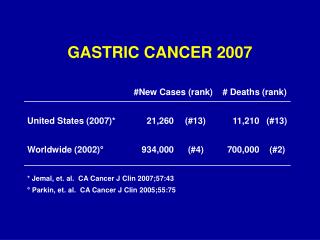
Gastric & Rectal Cancer D. Genovesi Radiation Oncology Department CHIETI www.radioterapia.unich.it. GASTRIC CANCER. GASTRIC CANCER. GASTRIC CANCER TNM Classifications AJCC. Gastric Cancer : Clinical Case Presentation PS: 100% (Karnofsky); 68 yrs old; male;

E N D
Gastric & Rectal Cancer D. Genovesi Radiation Oncology Department CHIETI www.radioterapia.unich.it
GASTRIC CANCER TNM Classifications AJCC
Gastric Cancer: Clinical Case Presentation PS: 100% (Karnofsky); 68 yrs old; male; Cardiac stroke 8yrs ago, no other diseases and no drugs at the moment. Endoscopy (17/12/2008): ulcer with free bottom and infiltrated margins at antropyloric region, increased thickness with non crossing stenosis. Contrast CT Thorax+abdomen (01/’09): negative lungs, liver and bones. Increased wall thikcness of gastric antrum (thickness of 2 cm) compatible with Eteroplasy. Concomitant small perivisceral nodes (0.5 cm) Bigger nodes at celiac region (2.1 cm); interaortocaval region (2.1 cm), paraortic region (1 cm). 05/01/’09: Sub-total gastrectomy+limphoadenectomy D2. Histology: Macroscopic: vegetant lesion of 4. 5 cm of antropyloric region at 1 cm from distal margin Microscopic: Carcinoma G3 (70%) and Adenocarcinoma G2 (30%) with entire gastric wall invasion. Free duodenal stump. Free proximal margin M+ of Carcinoma G3 in 1/14 lesser curvature nodes. No M+ in 22 greater curvature. No omental tumour. No M+ in retrocoledocus, retropancreatic, celiac, and left gastric artery nodes. PATHOLOGIC STAGE: p T2 p N1 M0 STAGE II
Key Points Diagnostic Work-up for Staging Prognostic Factors Surgical Treatment Neoadjuvant Treatments Adjuvant Treatments
Key Points Diagnostic Work-up for Staging • Double Contrast Upper G.I. • Barium Radiological Studies • Endoscopy: procedure of choice (8-10 biopsies) • Chest-Abdomen-Pelvic enhanced CT sensitivity 23-56% Early Gastric Cancer; 92-95% in advanced tumors metastatic lymph node: size criterion > 10 mm • Endoscopic Ultrasonography (EUS) • MRI has not achieved clinical importance • CT-PET: investigational procedure
Key Points Prognostic Factors • Tumor Grading ++ • R0; R1; R2 resection (operating procedure) +++ • T stage +++ • Lymphadenectomy ++++ at least 15 lymph nodes removed and analyzed Japanese Classification: 16 node stations in 3 groups depending on T • T location +++ proximal cancer poorer SVV vs distal cancer • Lymphatic, Venous or Perieneural invasion +++ • High CEA levels preop +
Key Points Surgical Treatment • Total Gastrectomy: proximal or middle third or diffuse T • Total Gastrectomy vs Subtotal Gastrectomy no advantage for distal (antral) Stomach • 5 cm free is required for resection margins • D1: perigastric LFN along lesser and greater curvatures (1-6) • D2: plus LFN along left gastric artery (7), common hepatic artery (8), celiac trunk (9), splenic hilus and splenic artery (10, 11) • D3:plus LFN along hepatoduodenal ligament (12), posterior surface of head of the pancreas (13) and the root of the mesentery (14) • D4:plus LFN paracolic region and abdominal aorta (15, 16)
Key Points Neoadjuvant Treatments • Preop Chemo: high risk pts (T3-T4; N0-2 M0); feasibility in Phase II studies (increase R0 rate); improve SVV in 4 Random Trials (ECF schedule); Type 2 Level of Evidence for Stages II-IV • Preop Radiotherapy (RT): benefit in only one random trial 40 Gy+S vs S Further Randomised Trials are required
Key Points Adjuvant Treatments • Postop Chemo: results often disappointing; poor compliance with multidrugs schedules; small-moderate benefit Type 2 Level of Evidence for Stages II-IV • Postop Radiotherapy (RT): No Benefit • Postop ChemoRadiotherapy: SWOG-INT 116, Stage I-IV, M0; Surgery + Obs vs CT-RT 5FU/L 5yrs OS: 40% vs 28.4% (p<0.001) 5yrs DFS: 31% vs 25% (p<0.001) 36% D1; only 10% D2 Kim et al: IJROBP 63, 2005: clinical benefit in D2 (SVV & DFS) Type 2 Level of Evidence for Stages II-IV
RESULTS 3 yr OS: 41% 48% 41% Macdonald JS et Al – New Eng J Med -2001
Kim IJROBP, 2005 Results DFS OS
Gastric Cancer: Clinical Case Presentation PS: 100% (Karnofsky); 68 yrs old; male; Cardiac stroke 8yrs ago, no other diseases and no drugs at the moment. Endoscopy (17/12/2008): ulcer with free bottom and infiltrated margins at antropyloric region, increased thickness with non crossing stenosis. Contrast CT Thorax+abdomen (01/’09): negative lungs, liver and bones. Increased wall thikcness of gastric antrum (thickness of 2 cm) compatible with Eteroplasy. Concomitant small perivisceral nodes (0.5 cm) Bigger nodes at celiac region (2.1 cm); interaortocaval region (2.1 cm), paraortic region (1 cm). 05/01/’09: Sub-total gastrectomy+limphoadenectomy D2. Histology: Macroscopic: vegetant lesion of 4. 5 cm of antropyloric region at 1 cm from distal margin Microscopic: Carcinoma G3 (70%) and Adenocarcinoma G2 (30%) with entire gastric wall invasion. Free duodenal stump. Free proximal margin M+ of Carcinoma G3 in 1/14 lesser curvature nodes. No M+ in 22 greater curvature. No omental tumour. No M+ in retrocoledocus, retropancreatic, celiac, and left gastric artery nodes. PATHOLOGIC STAGE: p T2 p N1 M0 STAGE II
GASTRIC CANCER: Management of our Clinical Case Day 1- Day 28-31 Day 56-58 Day 84-98 Day 112-6 FU-FA (5 gg) FU-FA (4 gg) FU-FA (3 gg) FU-FA (5 gg) FU-FA (5 gg) Radiotherapy INT-0116 Macdonald JS et Al – New Eng J Med -2001
Why preoperative treatments ? pCR R0 vs R+ Ajani JA et Al – JCO - 2005
RECTAL CANCER 11.000 – 12.000 new cases/year in Italy De Carli A., La Vecchia C. – 2002 Verdecchia A., Micheli A., Gatta G. – 2002
Rectal Cancer: Clinical Case Presentation PS: 100% (Karnofsky); 62 yrs old; male; no other diseases. Endoscopy (13/01/2006): ulcerated and vegetant lesion of 6 cm very near to internal anal sphincter HISTOLOGY: Adenocarcinoma G2. Contrast CT Thorax+abdomen (20/01/’06): negative lungs and liver. Neoplastic lesion which makes the lumen substenotic, presence of some lesions in perirectal adipous tissue.Two nodes of 1 cm in perirectal adipous tissue. CLINICAL STAGE: c T3 c N1 M0 IIIB STAGE
Key Points Diagnostic Work-up for Staging Pathology Surgical Treatment Radiotherapy and Chemotherapy Ongoing Research
Key Points Diagnostic Work-up for Staging • Endoscopy with biopsies • Endorectal ultrasound: T1 vs T2 tumors vs borderline T3 • Multislice-CT is not sufficiently accurate for low tumors CT cannot accurately distinguish LFN+ vs LFN- Phased Array MRI is highly accurate in Staging Difficulty in differentiation T1 vs T2 vs borderline T3 • Circumferential Resection Margin (CRM): MRI is highly accurate for the prediction of CRM • MRI with specific contrast enhanced (USPIO):promising • FDG-PET:disappointing results on N; role in response evaluation
The Circumferential Resection Margin predictivity MRI Sensitivity: 60-80%; Specificity: 73-100%
T3 with involved mesorectal fascia Beets-Tan et al. Lancet 2001 357 (9255) 497 - 504
Macroscopic assessment of Mesorectal excision CRM ( cm )% incomplete < 0.1 43.9 % 0.1 - 0.2 27.8 % 0.2 - 0.5 27.8 % 0.5 - 1.0 12.9 % > 1.0 11.1 %
Criterion for detection of node metastases No choice but to use the size of lymph nodes as the most reliable criterion In most cases, 5mm or larger, or 10mm or larger is regarded as criterion for lymph node metastases.
Metastatic nodes: less than Ø 5mm in > 50% Dworak et al. Surg Endos 1989;3:96-9 Brown et al. Radiology 2003;227:371-7
Key Points Pathology • Guideline and experience significantly improve the quality:www.rcpath.org/resources/pdf/colorectalcancer.pdf • Careful Macroscopic and Microscopic examination • Tumor Regression Grade (TRG) scales
Tumor-Regression-Grading: TRG Complete Regression (100%) Good Regression (> 50%) Moderate Regression (25-50%) Minimal Regression (< 25) No Regression (0%)
Key Points Surgical Treatment • The standard surgery: Total Mesorectal Excision (TME) • Preop Radio-chemoterapy + S: increase sphincter preservation (with good sphincter function) for downsizing • Pathological studies of CRM in anorectal junction and anal canal sphincter show higher rates of CRM involvement
Key Points Radiotherapy and Chemotherapy • Early T: local excision (adverse prognostic factors evaluation); endoluminal radiotherapy • c T3-4/N0 or plus: 15 Random Trials & 3 Meta-analysis: increase LC; conflicting results in SVV for preop Radiotherapy • Short-Course preop (5Gyx5) vs RT-CT: not seem effective for pts with predictive positive CRM e low tumor location • 2 Random Trials (EORTC 22921 & FFCD 9203) on role of chemo with preop-Radiotherapy: in RT-CT preop group increase of LC, increase rate of p T0, G3+ tox, no benefit of 5 yrs OS
Key Points Radiotherapy and Chemotherapy • Polish Trial in c T3-4: 5 Gy x 5 vs preop RT-CT: no difference in sphincter preservation, LC, OS but LATE TOXICITY • NCI Consensus Conference 1990: post-op CT-RT 5FU-based Standard treatment in post-op p T3/ p N1-2 rectal tumors • Preop RT-CT vs Post-op RT-CT 5FU-based: 4 Random Trials. The most important closed Trial is German Study CAO/ARO/AIO ‘94
P H A S E CAO/ARO/AIO 94 III Trial 50.4 Gy Bolus CI 5-FU Surgery 5-FU x 4 wks 1,5 T3 50.4 Gy Bolus Surgery CI 5-FU 5-FU x 4 wks 1,5
P H A S E CAO/ARO/AIO 94 III Trial Post-opPre-opP Evaluable # 394 405 - 5-Yr LF % 15 60.006 5-Yr Survival % 76 74 ns Acute toxicity 40 27 0.001 Chronic toxicity 24 14 0.012 5-Yr DF % 38 36 ns Sphincter Preservation 15/78 (20%) 45/116 (39%) 0.004 Sauer et al NEJM 2004
P H A S E CAO/ARO/AIO 94 III Trial The Value of Downstaging !!! C. Rödel et al., J Clin Oncol 2005; 23:8688-96
Key Points Radiotherapy and Chemotherapy • No data with level 1 evidence for adjuvant post-op chemo after preoperative RT-CT: it seems an effect of adjuvant chemo in responder pts • Unresectable rectal cancer: pre-op RT-CT 5FU-based to enhance R0 resectability (50-54 Gy Radiation dose) IORT: single institutions studies support a favourable effect • Local Recurrence: pre-op RT-CT +/- IORT (conflicting results); Re-irradiation is under clinical evaluation
Key Points Ongoing Research • Topic for surgical research: enhance organ preservation • Intensification of pre-op RT-CT and post-op chemo: - New Drugs (Oxaliplatin; Capecitabine) - Altered fractionation RT dose • EGFR and VEGF: promising targets of antitumor treatment • Individualised therapies based on clinical-pathological features and molecular and genetic markers • New Imaging for response evaluation
Rectal Cancer: Clinical Case Presentation PS: 100% (Karnofsky); 62 yrs old; male; no other diseases. Endoscopy (13/01/2006): ulcerated and vegetant lesion of 6 cm very near to internal anal sphincter HISTOLOGY: Adenocarcinoma G2. Contrast CT Thorax+abdomen (20/01/’06): negative lungs and liver. Neoplastic lesion which makes the lumen substenotic, presence of some lesions in perirectal adipous tissue.Two nodes of 1 cm in perirectal adipous tissue. CLINICAL STAGE: c T3 c N1 M0 IIIB STAGE
Rectal Cancer: management of our clinical case PLAFUR Schedule Follow-up 8 ws S 50.4 Gy CDDP 60 mg/mq 1° gg Chemo: N+ 5-FU 1000 mg/mq 1-5 gg
Ulcer Post CRT Pre CRT y p T0
Diffusion MRI PostCRT ypT0 PreCRT