Download
1 / 37
400 likes | 791 Views
Diseases of the Aorta. Armed Forces Academy of Medical Sciences. Outline. Aortic Aneurysms Thoracic Abdominal Risk Factors Treatment Aortic Dissection Presentation Risk factors Treatment. Thoracic Aorta. Anatomy Ascending aorta Aortic root & sinuses of Valsalva Aortic arch

E N D
Diseases of the Aorta Armed Forces Academy of Medical Sciences
Outline • Aortic Aneurysms • Thoracic • Abdominal • Risk Factors • Treatment • Aortic Dissection • Presentation • Risk factors • Treatment
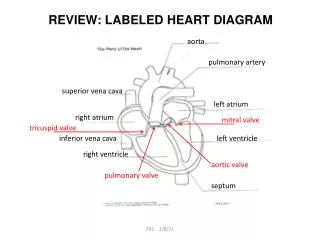
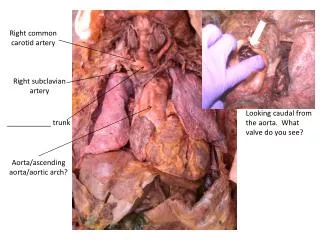
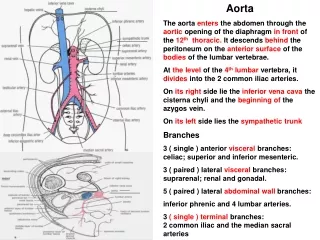
Thoracic Aorta • Anatomy • Ascending aorta • Aortic root & sinuses of Valsalva • Aortic arch • Great vessels: brachiocephalic, left common carotid, & left subclavian arteries • Descending aorta • Intercostal arteries • Anterior spinal artery • Abdominal aorta begins below diaphragm
Thoracic Aorta • Histology • Intima • Media • Adventitia • Physiology • Systole elastic stretch potential energy • Diastole elastic recoil kinetic energy
Aortic Aneurysm • Pathologic dilatation > 1.5 times the normal diameter • Fusiform = symmetric dilatation • Saccular = asymmetric out-poutching • Thoracic much less common than abdominal • AAA = 36.5 per 100,000 person-years • TAA = 5.9 per 100,000 person-years
Marfan syndrome AA & arch Ehlers-Danlos syndrome AA & arch Cystic medial degeneration AA & arch Atherosclerosis DA Traumatic Proximal DA Inflammatory Variable Infectious AA (syphilis) Variable (mycotic) Poststenotic AA (aortic stenosis) DA (coarctation) Postsurgical AA (s/p AVR) Etiology
Clinical Course • Natural history & progression of TAA not as well defined as AAA • Onset of symptoms heralds a more rapid course • Dichotomous growth rate • TAAs < 5.0 cm grow 0.17 cm/year • TAAs ≥ 5.0 cm grow 0.79 cm/year • 5-year survival = 20-50% • Rupture is most common cause of death
Clinical Presentation • Most abdominal and thoracic aneurysms are asymptomatic • Vascular complications • AR, CHF, ischemia from compression of coronary artery, sinus of Valsalva rupture into RA or RV with LR shunt, thromboembolism • Compression of external structures • SVC syndrome, dysphagia, hoarseness, respiratory complaints, chest or back pain • Rupture • Sudden, severe, sharp chest or back pain • Left pleural space > pericardium > esophagus
Physical Exam • Diastolic murmur of AR • Signs of CHF • Pulsatile mass in suprasternal notch (TAA) • Pulsatile mass infra-xiphoid (AAA) • Differential pulses in extremities • Signs of SVC syndrome (compression) • Decreased air movement or stridor (compression)
Diagnosis • CXR – shows widened mediastinum • CT – defines size & extent • MRA – also defines size & extent • TTE – limited use • TEE – role is under evaluation • Aortography – reserved for pre-op eval
Therapy • Medical • β-blockers decrease dP/dT (sheer stress) • Percutaneous • Stent graft for DA distal to left subclavian artery • Surgical • Recommended when maximal diameter is greater than 5.5 cm • 5 cm for Marfan or rapidly expanding patients
Surgery • Dacron tube graft • Bentall procedure = valve + graft • Survival • Perioperative mortality = 5-10% • 1-year survival ≥ 70% • 5-year survival = 50-60% • Complications • MI (7.2%), CVA (4.8%), ARF (2.4%), hemorrhage (7.2%), & paraplegia (6.0%)
Gadolinium-enhanced, three-dimensional MRA showing an aneurysm of the aortic arch (arrow) as well as a concomitant atherosclerotic ulcer (arrowhead) Krinsky G et al. N Engl J Med 1997;337:1475-1476
An 84-year-old man with a history of gastric cancer and hypertension was admitted to the emergency department in shock after loss of consciousness Kawasaki S and Kawasaki T. N Engl J Med 2007;356:1251
Aortic Dissection Pathophysiology • Tear in the intimal layer • Blood passes into aortic media through tear • Separates intima from surrounding media and adventita • Forms false lumen • False lumen can propagate proximally or distally
Aortic Dissection • Incidence = 2,000 cases per year in US • 2-to-1 male-to-female ratio • Peak incidence in 6th & 7th decade of life • 65% occur in AA, 20% in DA, 10% in arch, & 5% in abdominal aorta • Mortality (75-80%) is greatest during acute phase (< 2 weeks)
Classification of Aortic Dissection • DeBakey • 1: Originates in ascending aorta and propagates to at least the arch • 2: Originating in and confined to ascending aorta • 3: Originating in descending aorta • Stanford • More commonly used • Type A: Ascending aorta involvement regardless of site of primary tear • Type B: All other tears
Clinical Presentation • Sudden, severe chest and/or back pain • Tearing, stabbing, or ripping • Less common presentations • CHF (due to Aortic Regurgitation) • Syncope (due to tamponade) • CVA • Paraplegia (involvement of intercostal arteries) • Cardiac arrest
Physical Exam • Hypertension • Hypotension • Proximal dissection with tamponade • Diastolic murmur of AR • If dissection involves ascending aorta • Signs of CHF • Pulse deficits • If dissection involves left subclavian • Neurologic deficits • If dissection involves carotid arteries
Diagnosis • CXR • Widened aortic silhouette • Calcium sign = displacement of intimal calcium > 1 cm from outer aortic soft tissue • CT Angiogram • Sensitivity = 83-94% • Specificity = 87-100% • MRA • Gold standard • Sensitivity & specificity ~ 98%
Diagnosis • Transthoracic Echocardiogram • Better for AA than DA • Sensitivity = 59-85% • Speficificty = 63-96% • Transesophageal Echocardiogram • Sensitivity = 98-99% • Specificity = 77-97% • Depends on experience of operator
CT Scan Showing Localized Dissection of the Aortic Arch with an Intimal Tear (Arrows) Pasic M et al. N Engl J Med 1999;341:1775
TEE of type A aortic dissection O'Gara P et al. N Engl J Med 2004;350:1666-1674
TEE for Aortic Dissection www.uptodate.com
Treatment of Aortic Dissection Nienaber CA, Eagle KA. Circulation 2003; 108: 772-778.
Acute Treatment of Aortic Dissection • Immediate Heart Rate control • Labetalol • Propranolol • Goal HR < 60 bpm • Immediate blood pressure control • Nitroprusside • Nitroglycerine • Goal MAP 60-70 mmHg • Pain control
Definitive Therapy for Aortic Dissection • Type B (confined to descending aorta) • Medical therapy: control HR and BP • Surgical therapy: only for complicated course • Occlusion of major arterial branch • Extension of dissection flap • Type A (involves ascending aorta) • True surgical emergency
Intramural Hematoma • Thrombus between intima & adventitia • Typically occurs in elderly patients with hypertension • Precursor for aortic dissection • 15-20% of dissections present with hematoma • 12-45% of hematomas progress to dissection • Managed similarly to aortic dissection
Computed Tomographic Scan of an Intramural Hematoma (Arrows) of the Ascending Aorta Kouchoukos N and Dougenis D. N Engl J Med 1997;336:1876-1889