Download
1 / 46
510 likes | 1.36k Views
Heart Disease Braunwald. CV R4 李威廷醫師 Supervisor: 李貽恆醫師. Diseases of the aorta. Aorta . Intima, media, adventitia ascending, arch, descending Aortic isthmus: arch-descending junction. Aortic aneurysm.

E N D
Heart Disease Braunwald CV R4 李威廷醫師 Supervisor: 李貽恆醫師 Diseases of the aorta
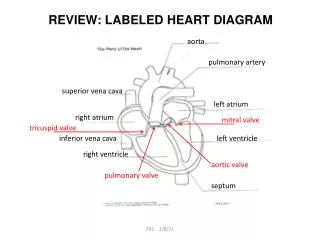
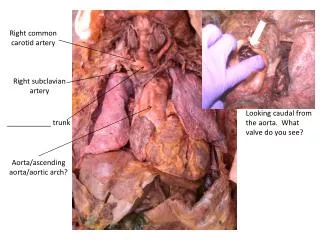
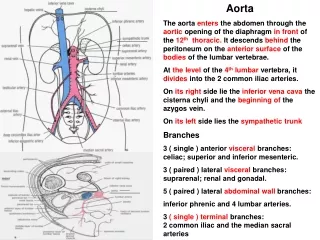
Aorta • Intima, media, adventitia • ascending, arch, descending • Aortic isthmus: arch-descending junction
Aortic aneurysm • Definition: pathological dilatation of the normal aortic lumen involving one or several segments • Fusiform (common), saccular • Pseudoaneurysm: well-defined collection of blood and connective tissue outside the vessel wall
Abdominal aortic aneurysm • Age (M>55 y/o; F>70 y/o) • Atherosclerosis • Infrarenal arota: no vasa vasorum at media • Gene (Marfan, Ehlers-Danlos syndrome) • Prevalence: >3% • Aneurysm rupture: 80% into left retroperitonium cavity
Abdominal aortic aneurysm • Pain: most common, at hypogastrium or back, not affected by movement • Asymptom • Rupture triad: abdominal or back pain; palpable/ pulsatile abdominal mass; hypotension (<1/3 cases) • Bruit (+/-) • Abdomianl echo, CT, MRA, aortography
Abdominal aortic aneurysm • Surgical indication: rupture; size >4—5 cm; expanding rapidly (>0.5 cm/year) • Coronary angiography • Medication control: Hyperlipidemia, hypertension, cigarette smoking • CT follow up every 3—6 months
Thoracic aortic aneurysm • Descending aorta > ascending aorta • Cystic media degeneration: weakening aortic wall (elastic fiber degeneration) • Marfan syndrome: autosomal dominant • Ahterosclerosis • Syphilis: ascending aorta • Infectious aortitis / mycotic aneurysm
Thoracic aortic aneurysm • 40% asymptom, pain • A-V shunt, superior vena cava syndrome (mass effect), tracheal deviation, hematemesis • CT, TEE > TTE • Surgery: >5cm (mean expansion rate= 0.43 cm/year) • Op risk: 5%
Thoracic aortic aneurysm • Annuloaortic ectasia: elastic fiber degeneration + aortic regurgitation • Aortic valve replacement
Aortic dissection • Tear in aortic intima • Antegrade, retrograde • false lumen, intimal flap, true lumen • Acute (2/3), chronic (1/3) • Ascending (65%), arch (20%), descending thoracic (10%), abdominal (5%) • Mortality: 1% per hour
Aortic dissection • Peak: 60—70 y/o • Hypertension, bicuspid aortic valve • Marfan syndrome (cystic media degeneration) • 3rd trimester pergnancy • Blunt trauma • IABP • Prior cardiac surgery
Aortic dissection • Severe tearing pain (sudden onset), CHF, syncope, CVA, ischemic peripheral neuropathy, paraplegia, cardiac arrest, sudden death • Anterior pain only: 90% ascending • Interscapular pain only: 90% descending
Aortic dissection • Hypertension (descending), hypotension (ascending) • Pseudohypotension (involving brachiocephalic vessel) • Pulse deficit (transient), AR, neurological finding (proximal, conscious level or spinal cord ischemia) • AMI (RCA > LCA) • Pleural effusion (left side), cardiac tamponade • Horner syndrome
Aortic dissection • Calcium sign: 1.0cm (suggestive, not diagnostic) • Normal CXR cannot exclude dissection • EKG: LVH (1/3); absence of ST and T change; AMI (involving coronary a.) • Initial diagnosis rate: 62%
Aortic dissection • Mortality: 25% (<24h), 50% (1w), 75% (1m), 90% (1y) • BP favor RA • BP on LA if higher BP in LA than RA • SBP: 100—120mmHg, • mean BP: 60—75mmHg • Pain control, beta-blocker, nitroprusside, ACEI • Hypotension: prefer levophed • Pericardiocentesis for cardiac tamponade
Atypical aortic dissection Intramural hematoma: • rupture of vasa vasorum, • aortic dissection without intimal flap, • 10% type B dissection, • failed diagnosis in aortography, • high risk for aneurysm formation, • medication (distal) or surgery (proximal)
Atypical aortic dissection Penetrating atherosclerotic ulcer: • old, hypertension • no false lumen, • Aortography is standard • no definite treatment
Aortic atherothrombotic emboli • Age, hypertension, DM, hyperlipidemia, vascular disease • Most common in descending thoracic aorta • Coumadin is for high risk patients to prevent embolic event • Post-operative stroke
Cholesterol embolization syndrome • Cholesterol crystal from ulcerated atheromatous plaques • “blue-toe” or “purple-toe” syndrome • Elevated ESR & eosinophil • Reduced complement level • No specific therapy
Acute aortic oolusion • Infrarenal aorta at bifurcation • Saddle embolus • Af / RHD, MI, DCM, aneurysm • Bilateral leg pain, weakness, numbness, paresthesia, • Cold, cyanosis, absent pulse, diminished or absent deep tendon reflexes • Aortogram • Heparin, transcatheter, operation • life-long anticoagulant
Primary tumor of aorta • < 50 Cases • Equal in thoracic and abdomen aorta • Back pain • Aortography, biopsy • Prevent embolization
Heart Disease Braunwald Zipes Libby sixth edition, 2001 CV R4 李威廷醫師 Supervisor: 李貽恆醫師 Jul 1st , 2004 Peripheral artery diseases
Peripheral artery diseases < 60 y/o population: <3% > 75 y/o population: >20%
Peripheral artery diseases Intermittent claudication: • pain, ache, fatigue, or discomfort in the affected leg during exercise, particularly walking (oxygen demand) • resolved with rest within few minutes • Buttock, hip, thigh • Gastrocnemius muscle is most common • Walking Impairment Questionnaire • Arterial embolism, vasculitis / arteritis, secondary compression, lumbar sacroradiculopathy (neurogenic pseudoclaudication, standing)
Peripheral artery diseases Rest pain • Inadequate blood flow • Skin fissure, ulceration, or necorsis • DM neuropathy or ischemic neuropathy
Peripheral artery diseases Physical examination: • Absent pulse distal to the stenotic site • Bruit of the stenotic site • Muscle atrophy, hair loss, cool skin, poor healing, pressure sore,
Peripheral artery diseases Ankle/brachial index (ABI): • SBP ratio (normal: >=1) • ABI <0.9 : 95% sensitive for PAD • ABI 05—0.8 with claudication: critical limb ischemia • ABI <0.5 or ankle BP <55mmHG: poor ulcer healing MR angiography: 95% sensitivity and specificity Contrast angiography
Peripheral artery diseases—treatment Risk factor modification Control DM, HTN, smoking cessation Antiplatelet therapy: ticlopidine, plavix Exercise: improve maximal walking distance than PTA Angioplasty / stents and surgery • Trental: RBC flexibility and anti-inflammatory • Pletal: unknown • Beta-blocker: controversial
Thromboangitis obliterans • Young smokers • Medium and smalll vessels of the arms • Cause unknown? Type I and III collagen • Pain, digit ulceration, Raynaud phenomenon • Abnormal allen test (2/3) • Tx: Cessation smoking, prostacyclin analogue,
Acute limb ischemia • Arterial embolism (Af) • thrombosis with plaque ruprure • dissection, • trauma