Download
1 / 25
280 likes | 397 Views
Diseases of aorta. Jakub Honěk Kardiologická klinika 2.LF UK a FN Motol. Overview. Anatomy and physiology Abdominal aortic aneurysm (AAA) Aneurysm of thoracic aorta Aortic dissection. Anatomy. Ascending aorta Aortic root ST junction Tubular part Aortic arch Aortic isthmus

E N D
Diseasesof aorta Jakub Honěk Kardiologická klinika 2.LF UK a FN Motol
Overview • Anatomy and physiology • Abdominal aortic aneurysm (AAA) • Aneurysm of thoracic aorta • Aortic dissection
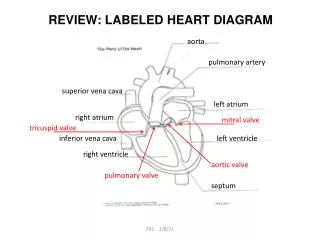
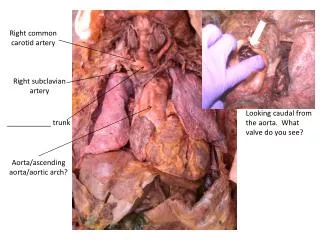
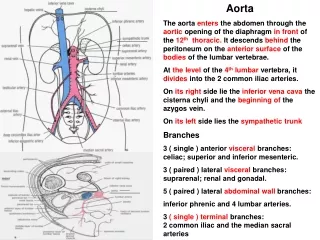
Anatomy • Ascending aorta • Aortic root • ST junction • Tubular part • Aortic arch • Aortic isthmus • Descending aorta • Abdominal aorta • Suprarenal segment • Infrarenal segment • Bifurcation
PhysiologyArterialstiffness Zieman SJ. Arterioscler Thromb Vasc Biol 2005;25:932-943.
AAA • Localizeddistension • ofaorticdiameter>50% (>3.0cm in women, >3.4 cm in men) • 90 % subrenal • Progressesovertime • 5x more frequent in men • Prevalence ↑withage • Multifactorial etiology • Risk factorssimillar to atherosclerosis, pathophysiologyisdifferent - aorticwallremodelling
AAAClinicalfeatures • Mostlyasymptomatic! • Rarelypatientpalpatespulsatilemass, orfeelspulsations • Mostlyfirstsmyptomsoccurdue to complications • Peripheralthromboembolism • AAA rupture (first sign in 40%!)
AAA rupture • Emergent, lifethreateningsituation • Mortality 80–90 % whenoptimallytreated • 90% retroperitonealrupture • Clinicaltriad • PAIN (amdominal/lumbar, radiation to groins) • PULSATILE MASS • HYPOTENSION (circulatoryshock)
AAA diagnosticimaging • Duplex ultrasound • Fast, cheap, screeningofpts. in risk, follow-up • CTA/MRA • Optimalresolution, anatomy • DSA • Invasivetreatment, luminography • Screening • Effective in risk groups (pts. Withfamilyhistory, CAD, PAD, male smokers>65 yrs…) • Preventionoffatalcomplications, electiveoperation/inetervention
Treatment – stable AAA • Lifestylechanges, follow-up, bloodpressurecontrol (beta-blockers) • Preventiveoperation/intervention Indicationbased on AAA diameter: > 55 mm > 10 mm increase/year Modifiedby BSA, sex, comorbidities
Treatment – stable AAA • Surgery • Resection of aneurysmal sac, implantation of vascular prosthesis • Endovascular treatment • Implantation of stentgraft • Femoral approch • Simila longterm results to surgery • Conservative • Follow-up, risk of rupture
Treatment – ruptured AAA • Emergent surgery/endovascular tretament • Patient stabilization, fast imaging • Up to 50% pts. die before reaching hospital • 30-40% die die before reaching op. Theatre • 40-50% of the operated die • Overall mortality 80-90%
Aneurysmofthoracic aorta • Lessfrequentthan AAA (10/100 000) • Same definition • 60% ascending, 5-10% arch, 30-35% descendning • Anuloaortic ectasia
Aneurysmofthoracic aorta • Multiple etiologies – genetic, degenerative, infectious, inflammatory • Bicuspid aortopathy • Cystic medial degeneration • Mostly assymptomatic • Symptoms of complications: Ao regurgitation, embolization, compression sy., dissection, rupture • Iamging: TTE, TEE, CTA, MRA, DSA
AneurysmofthoracicaortaTreatment • BP control • Follow-up • Elective surgery Bonow et al. Braunwalds heart disease.
Aorticdissection • Incidence: 3/100 000 per year • High mortality • Untreated: 25%/24h, 50%/week • Optimal treatment: 20%/30 days • Intimal tear – entry • Intimal flap, false lumen • Reentry
AorticDissection - classification Stanford De Bakey Entry: 65% root, 20% isthmus, 15% other
AorticdissectionClinicalmanifestation • Pain • severe, sudden, sharp – stabbing, tearing („stabbed in the chestwhit a knife“) • Retrosternal (+radiation to neck, jaw), between scapulae, abdominal, back • Acute heart failure, MI, syncope, stroke, paraplegia…
AorticdissectionDiagnosticapproach • Urgent situation – fast diagnosis • Rare disease vs. Common diseases • Physical exam, ECG, lab (D dimers) • Ideal imaging test – fast, available, good resolution – CTA • Trasthoracic echo - bediside
AorticdissectionTherapy • Urgent situation, high mortality in first hours • Multidisciplinary approach • Initial management: • BP control (beta blockers) • Pain control • Hemodynamic stabilization • In type A – plan urgent surgery • In type B – conservative/ surgery/endovascular