Download
1 / 8
80 likes | 218 Views
What is the Marginal Cost-Effectiveness of EBCT in an Asymptomatic Screening Population? ( Compared to Conventional Risk Prediction). Allen J. Taylor MD,FACC Prospective Army Coronary Calcium (PACC) Project Walter Reed Army Medical Center, Washington, D.C.

E N D
What is the Marginal Cost-Effectiveness of EBCT in an Asymptomatic Screening Population? (Compared to Conventional Risk Prediction) Allen J. Taylor MD,FACC Prospective Army Coronary Calcium (PACC) Project Walter Reed Army Medical Center, Washington, D.C. Uniformed Services University, Bethesda, MD
Background • Risk factors underestimate CVD risk • Screening EBCT Rationale: • Risk of CVD (4-fold) if Ca+ present • High % are “low risk” by risk factors • Potential to capture misclassificatied risk • Costs of screening for sub-clinical CVD are poorly understood
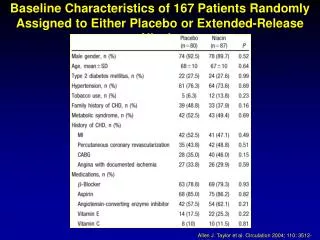
Base Case Assumptions • Life Expectancy (for average 40yo, 80%M) • “At Risk”: 35 years • “Low Risk”: 40 years • Utility of taking medications • 0.98 • Efficacy of Primary Prevention • 30% RRR in mortality • EBCT CAC increases RR by 4
ResultsCost Per Quality-Adjusted Life Year • $90,000 per QALY for base case • “Expensive” by conventional standards • Most sensitive to the • Efficacy of primary prevention • Utility of taking life-long medications • Independent prognostic value of EBCT
Tornado Diagram of Important Variables Efficacy of Primary Prevention 50% RR 10% RR Utility on Medication 0.99 0.90 Incidental Finding 2% 20% Cost of Medications $100 $600 Cost of EBCT $800 $200 10K 90K 200K +
Limitations • Cost per case identified difficult to interpret • $$ per QALY requires many assumptions • Efficacy of risk identification not truly known • Prognostic value of calcification above conventional risk factor modeling is still controversial • Modeled 40yo asymptomatic population only • May not be generalizable to older populations
Conclusions • EBCT identifies a substantial number “at risk”, at a cost of $2990 per additional “at risk” case • The marginal COST/QALY is dependent on: • Value of CAC over FRI (>4-fold) • Cost and utility of medication (< $300/yr) • Incidental findings on EBCT (< 10%) • Efficacy of primary prevention (> 25% RRR) • Our base case using favorable assumptions indicated EBCT screening costs $75,000/QALY
Implications • Health systems, insurers and society need to understand the costs of new technologies that screen for coronary disease • Modeling can help assess the added value (or harm) of new technology where there is substantial uncertainty