Download
1 / 36
• 570 likes • 1.42k Views
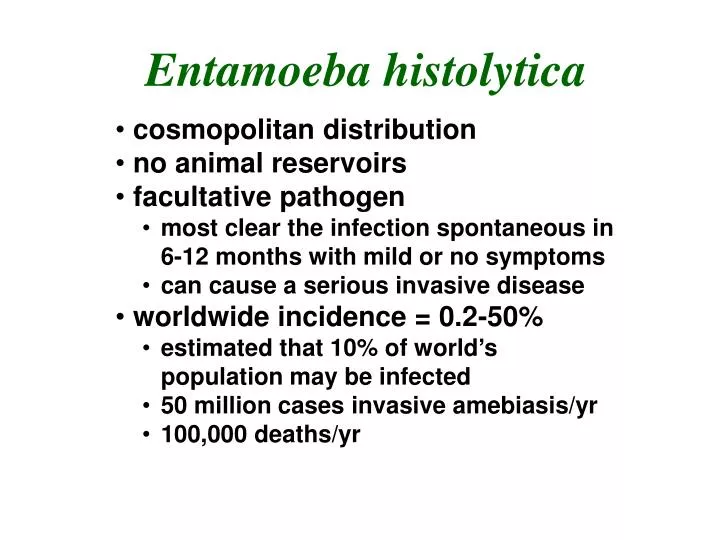
Entamoeba histolytica. cosmopolitan distribution no animal reservoirs facultative pathogen most clear the infection spontaneous in 6-12 months with mild or no symptoms can cause a serious invasive disease worldwide incidence = 0.2-50% estimated that 10% of world’s population may be infected

E N D
Entamoeba histolytica • cosmopolitan distribution • no animal reservoirs • facultative pathogen • most clear the infection spontaneous in 6-12 months with mild or no symptoms • can cause a serious invasive disease • worldwide incidence = 0.2-50% • estimated that 10% of world’s population may be infected • 50 million cases invasive amebiasis/yr • 100,000 deaths/yr
Facultative Pathogenicity of Entamoeba histolytica • 1875 Lösch correlated dysentery with amebic trophozoites • 1925 Brumpt proposed two species: E. dysenteriae and E. dispar • 1970's biochemical differences noted between invasive and non-invasive isolates • 80's/90's several antigenic and DNA differences demonstrated • rRNA 2.2% sequence difference • 1993 Diamond and Clark proposed a new species (E. dispar) to describe non-invasive strains • 1997 WHO accepted two species
Entamoeba histolytica Life Cycle
Excystation • cyst wall disruption • ameba emerges • nuclear division (48) • cytoplasmic division (8 amebala) • trophozoites colonize large intestine • feed on bacteria and debris • replicate by binary fission
Excystation • cyst wall disruption • ameba emerges • nuclear division (48) • cytoplasmic division (8 amebala) • trophozoites colonize large intestine • feed on bacteria and debris • replicate by binary fission
Encystation • trophozoite rounds up • secretion of cyst wall • aggregation of ribosomes (= chromatoid bodies) • 2 rounds of nuclear division (14 nuclei) • survive weeks to months
immature cyst mature cyst trophozoite
Pathogenesis of Amebiasis • NON-INVASIVE • ameba colony on intestinal mucosa • asymptomatic cyst passer • non-dysenteric diarrhea, abdominal cramps, other GI symptoms • INVASIVE • necrosis of mucosa ulcers, dysentery • ulcer enlargement dysentery, peritonitis • metastasis extraintestinal amebiasis
ulcers with raised borders • little inflammation between lesions
‘flasked-shaped ulcer’ • trophozoites at boundary of necrotic and healthy tissue • trophozoites ingesting host cells • dysentery (blood and mucus in feces)
localized sloughing • ulcers coalesce • perforation of intestinal wall Lateral and Downward Expansion of Ameba into Lamina Propria
Disease Manifestations • ulcer enlargement severe dysentery • perforation of intestinal wall peritonitis • local abscesses • 2o bacterial infections • occasional ameboma (=amebic granuloma) • cessation of cyst production ameboma = inflammatory thickening of intestinal wall around the abscess (can be confused with tumor)
Extraintestinal Amebiasis • metastasis via blood stream • primarily liver (portal vein) • other sites less frequent • ameba-free stools common • high antibody titers • Amebic Liver Abscess • chocolate-colored ‘pus’ • necrotic material • usually bacteria free • lesions expand and coalesce • further metastasis, direct extension or fistula
Pulmonary Amebiasis • rarely primary • rupture of liver abscess through diaphragm • 2o bacterial infections common • fever, cough, dyspnea, pain, vomica
Cutaneous Amebiasis • intestinal or hepatic fistula • mucosa bathed in fluids containing trophozoites • perianal ulcers • urogenital (eg, labia, vagina, penis)
Cutaneous Amebiasis • intestinal or hepatic fistula • mucosa bathed in fluids containing trophozoites • perianal ulcers • urogenital (eg, labia, vagina, penis)
Cutaneous Amebiasis • intestinal or hepatic fistula • mucosa bathed in fluids containing trophozoites • perianal ulcers • urogenital (eg, labia, vagina, penis)
Facultative Pathogenicity • 85-90% of infected individuals are asymptomatic • ~10% of the symptomatic will develop severe invasive disease
Molecular Epidemiology • molecular probes used to survey for E. dispar and E. histolytica • E. dispar ~10-fold > E. histolytica • discrete endemic pockets of E. histolytica • many asymptomatic E.h. infections • ~10% of the E.h. infections are associated with invasive amebiasis • ~25% seropositive for E. histolytica in endemic areas
a pathogen has an inherent ability to break host cell barriers • virulence usually correlates with ability to replicate within host • various degrees of virulence may be exhibited depending on conditions
contact-dependent killing of epithelial cells • breakdown of tissues (extracellular matrix) • secreted proteases? • contact-dependent killing of neutrophils, leukocytes, etc.
Galactose Inhibitable Adherence Protein • trophozoites adhere to mucins, epithelial cells, leukocytes, etc • mediated by galactose-inhibitable lectin activity • lectin activity due to surface protein (GIAP) • 170 kDa heavy chain mediates binding (multigene family) • 35 kDa light chain anchor to membrane • a-GIAP Abs abrogate complement resistance • ~85% identity between Eh and Ed • Are there differences in adherence? • after contact the target cell is lysed and phagocytosed by the trophozoite
Host Cell Lysis and Phagocytosis • Amebapore • pore-forming peptide • potent anti-bacterial activity • located in vacuoles, not secreted • Eh and Ed sequences are 95% identical • GluPro change breaks a-helix • Ed had 80% less activity than Eh
Entamoeba Proteases • Eh expresses and secretes higher levels of cysteine proteases • 6 cys-protease genes (ehcp1-6) • ehcp1 and 5 are missing in Ed • 90% inhibition of ehcp5 did not affect trophozoite mediated destruction of host cell monolayers
Intestinal Symptoms • range • mild to intense • transient to long lasting • nondysenteric • diarrhea • cramps • flatulence • nausea • dysenteric • blood/mucus in stools • cramps/pain • tenesmus • ameboma • palpable mass • obstruction
Control and Epidemiology Treatment • asymptomatic • iodoquinol or paromomycin • endemic areas? • symptomatic • metronidazole or tinidazole • followed by lumenal agents • drain liver abscess • only with high probability of rupture! • avoid fecal-oral transmission • not normally associated with travelers diarrhea • > 1 month stay • institutions • mass drug treatment little affect • staff and improved housing conditions lowers prevalence • male homosexuals • 40-50% in NYC and SF during late 70’s • lower since AIDS/safe sex