Download
1 / 23
230 likes | 259 Views
Explore the challenges of oesophageal injuries like perforation, Boerhaave syndrome, and diagnostic techniques. Learn about underlying disorders, clinical presentations, and common misdiagnoses requiring urgent surgical intervention.

E N D
Oesophagealemergencies Pál Ondrejka Professor of Surgery
Emergencyoeasophagealdisorders • Perforation • Iatrogenicperforation • Spontaneousperforation • Boerhaave’ssyndrome • Traumaticperforation • Blunt trauma • Penetratinginjuries • Foreign body • Causticinjuries • Alcalic • Acidic
Whytheoesophagealinjuriesarehighlyproblematic? • The proximity of vitalstructures • The bloodsuply • The lack of serosalsurfacearroundtheorgan • The injuriesarecarryhighmorbidity and mortality • Most surgeons has limited experienceswithdiagnosis and treatment of suchcases
Boerhaave syndrome • Boerhaave first described Boerhaave syndrome, which involves tearing of the oesophagus, usually a consequence of vigorous vomiting. He notoriously described in 1724 the case of Baron Jan van Wassenaer, a Dutch admiral who died of this condition following a gluttonous feast and subsequent regurgitation.[8] This condition was uniformly fatal prior to modern surgical techniques allowing repair of the oesophagus.
Aetiology • Suddenrise of intra-abdominalpressure (80-90%) • Vomitingorretching • Blunt trauma • Weightlifting • Defecation • Heimlich manoeuvre • Status epilepticus
Existingunderlyingoesophagealdisorders (10-20%) • Malignancy • Pepticulceration • Herpessimplexvirus (HSV) • Human immunodeficiencyvirus (HIV) • Tuberculosis (TB)
Tipicallocation • Justabovethediaphragm • Leftposterolateralposition • Usuallysingl, longitudinal, 1-8 cm • Men : women = 4 . 1 • Medianage 64 years • Most of thambecauseofalcoholicintoxication • Pleuraldisruptiondevelopesbarogenicallyorfrom rapid gastricaciderosion
Mackler’striadofclinicalpresentation of oesophagealperforation • Vomitingorretching • Chestpain (Sudden and dramatic) constant, epigastricorretrosternal, exacerbatedbymovement • Subcutaneousemphisema (takesabout an hourtodevelop)
Othersymptomes • Tachycardia, tachypnoe • The patienttakessitingpositioninordertoreducediaphragmaticmovements • Patientsarepale and sweaty • Coolperipheries • Chemicalpleuromediastinitisdevelops • In 24.48 hourscardiopulmanaryinsuffitientydevelops
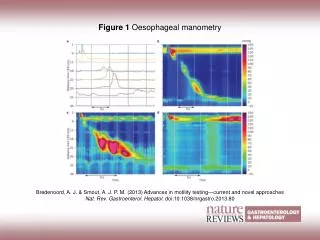
Diagnosticexaminations • Plainchest and abdominalradiography • Contrastradiography • Uppergastrointestinalendoscopy • Computedtomography (CT) • Other • Pleuralaspiration • Oralbluedyes
Tipicalchestradiographyfindings • Pleuraleffusion • Pneumomediastinum • Sucutaneousemphysema • Hydropneumothorax • Pneumothorax
Preoperativeresustitation • Control of airway and administration of O2 • Earlyanaestheticinvolvment • Stabilecentralintravenosusaccess • Urethralcatether • Broadspectrumantibiotic and antifungalagents • Intravenosusantisecretorydrugs • Zerodiet • Intercostalchestdrainage • Nasogastrictube
Frequentmedicalmisdiagnoses • Myocardialinfarction • Pericarditis • Spontaneouspneumothorax • Pneumonia • Oesophagealvarices/mallory-Weistear • Mesentericischaemia
Frequentsurgicalmisdiagnoses • Peritonitis • Acutepancreatitis • Perforatedpepticulcer • Renalcoloc • Aorticaneurism (dissection/rupture) • Billiarycolic • Mesentericischaemia