Download
1 / 38
380 likes | 689 Views
ANOTHER LUMP IN THE NECK Amanda Brown, is a 35 year old primary school teacher. She has a history of pancreatitis, and no medication except the oral contraceptive pill. She smokes 10 cigarettes/day. The G.P, Dr Black records for this problem are as follows:

E N D
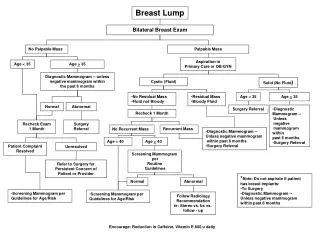
ANOTHER LUMP IN THE NECK Amanda Brown, is a 35 year old primary school teacher. She has a history of pancreatitis, and no medication except the oral contraceptive pill. She smokes 10 cigarettes/day. The G.P, Dr Black records for this problem are as follows: 3rd October: Dry cough and (?) slight breathlessness Chest and throat clear on examination, PEFR = 420 l/min Advised symptomatic treatment (fluids, paracetamol, aspirin gargles) Told to stop smoking 11th Nov: Returns to GP - cough worse, keeping her awake at night. No sputum. She has now developed chest pain. She is complaining of feeling hot at night and has lost 6kg in weight O/E: Temperature 38.20C Rubbery non-tender 2cm lymph node in left anterior triangle of neck How would the GP have examined the neck? Consider the differential diagnosis for an enlarged lymph node in the neck. What is the procedure for urgent assessment in this situation?
Things to consider • Differential diagnosis in relation to • Her age • Her symptoms • Characteristics of the neck lump • Causes of lumps in the neck • Which investigations ?
Causes of enlarged lymph nodes • Age: node biopsies showing malignancy • 20%<20y • 80%>50y • Characteristics of the lump • Size • Location eg supraclavicular v post cervical • Tender nodes less likely to be malignant • Matted/fixed adherent more malignant • BIOPSY TO BE SURE
Differential diagnosis of lumps in neck • Acute infection • bacterial, viral • Chronic infection • mycobacterial, toxoplasmosis • Inflammatory process • granulomatous disease • Malignant process • primary or secondary? • Other causes • Developmental cysts • Lipoma • Nodular goitre
Investigations at this stage GP might consider: • Serological testing: HIV, EBV (monospot) • Full blood count • Biochemical testing: LFT, LDH • Chest X-ray • Referral to rapid access neck lump clinic
Neck lump clinic • Recommendation of cancer network • Rapid access: ENT assessment +FNA/Biopsy • FNA: may help to distinguish if infective or malignant • Biopsy: best for establishing diagnosis of lymphoma/other malignancy
Dr Black refers her urgently to the local neck lump clinic. She is given an appointment for the following week. However, before then her chest pain becomes more severe and she attends the A&E Department. She is more breathless and finds it difficult to lie flat. She is admitted to hospital. A chest X-Ray is reported as showing a mediastinal mass with left paratracheal nodes What differential diagnosis should be considered by the doctor in A&E? Which urgent investigations should be requested?
Causes of chest pain and breathlessness in this context • Infection • Pulmonary embolism • Pleural effusion • Malignant infiltration of lungs/heart • Pericarditis • Pulmonary oedema • Mass effect History and clinical findings will help differentiate cause Investigations: Chest X ray, FBC
Causes of a Mediastinal Mass on CXR • Anterior mediastinum • Thymus • Lymphoma • Pericardial cyst • Thyroid, parathryroid • Middle mediastinum • Bronchial carcinoma • Lymphoma • Infectious process • Metastatic node • Posterior mediastinum • Vascular lesion • Neurogenic tumour • Lymphoma
An opinion is sought from Dr White, the Haematologist. She recommends a lymph node biopsy. Amanda is worried about scarring to the neck and asks if there is an alternative method of getting a result. Dr White tells her that a complete lymph node biopsy will be necessary to obtain the diagnosis and that other investigations are also necessary What methods are used to get tissue from lymph nodes? Which is the most suitable in this case? What other investigations are required?
Best practice in lymphoma diagnosis and reporting(BCSH 2007) Recommendations • Fine needle aspiration samples should not normally be used as the sole tissue for diagnosis (Grade B; evidence level III) • “Lymph node biopsies should be taken whenever possible. Core biopsies may be necessary from inaccessible sites but it is recognised that diagnoses where architecture is important e.g indolent lymphomas may be difficult” • Each MDT should have at least one identified Pathologist who will review material from all new diagnoses (Grade C; evidence level IV) www.bcshguidelines.co.uk
Investigations • CT Thorax • Lymph node biopsy • consider Thoracoscopy and mediastinal biopsy if no peripheral nodes • FBC • Renal, Liver function, Lactate Dehydrogenase (LDH) • Echocardiogram • HIV serology
The biopsy is reported as showing Diffuse Large Cell Non-Hodgkin’s Lymphoma (DLBCL). Dr White sees Amanda with the Joanne Green the haematology Specialist Nurse to explain the diagnosis and treatment. Dr White informs her that her case will be discussed at the Lymphoma MDT where a complete treatment plan will be made and she will discuss the results with her. She also outlines the benefits and risks associated with treatment and possible long term side effects. Joanne Green stays behind to talk further to Amanda and gives her a information booklets on NHL, chemotherapy and consent to treatment. The nurse reports that Amanda’s main concern are the possible effects on fertility as she would like to have children, although does not have a partner at the present time.
Questions: • Why/how to we stage Non – Hodgkin’s Lymphoma? • What are the implications of being diagnosed with this condition? • What are the side effects of chemotherapy? • What is the role of the multidisciplinary team in managing cancer? • What sources of patient information are available?
Lymphoma • Malignancy of cells of lymphoid origin • The major subdivision is Hodgkin's Lymphoma (HL) and Non Hodgkin's Lymphoma (NHL) – histologically distinct • The incidence of lymphomas compared to leukaemias • ~ 500 cases of CML in UK annually • ~2,500 cases of AML in UK annually • 7,500 cases of NHL in UK annually • 1,200 adult cases of HL UK annually Hodgkin’s Lymphoma • Differs clinically from NHL • Characteristic Reed-Sternberg cells found which are not usually present in NHL
Classification of Lymphoma WHO classification of lymphoma (2001) • Cell lineage i.e. B, T /NK • Morphology • Immunophenotype • Clinical behaviour • Genetic features Defines specific disease entities allowing tailored treatments and indications of prognosis
B-Cell Neoplasms Precursor B-cell neoplasm Precursor B-lymphoblastic leukemia/lymphoma (precursor B-acute lymphoblastic leukemia) Mature (peripheral) B-neoplasms B-cell chronic lymphocytic leukemia / small lymphocytic lymphoma B-cell prolymphocytic leukemia Lymphoplasmacytic lymphoma‡ Splenic marginal zone B-cell lymphoma (+ villous lymphocytes)* Hairy cell leukemia Plasma cell myeloma/plasmacytoma Extranodal marginal zone B-cell lymphoma of MALT type Nodal marginal zone B-cell lymphoma (+ monocytoid B cells)* Follicular lymphoma Mantle cell lymphoma Diffuse large B-cell lymphoma Mediastinal large B-cell lymphoma Primary effusion lymphoma† Burkitt’s lymphoma/Burkitt cell leukemia§ T and NK-Cell Neoplasms Precursor T-cell neoplasm Precursor T-lymphoblastic leukemia/lymphoma (precursor T-acute lymphoblastic leukemia ‡ Formerly known as lymphoplasmacytoid lymphoma or immunocytoma II Entities formally grouped under the heading large granular lymphocyte leukemia of T- and NK-cell types * Provisional entities in the REAL classification Mature (peripheral) T neoplasms T-cell chronic lymphocytic leukemia / small lymphocytic lymphoma T-cell prolymphocytic leukemia T-cell granular lymphocytic leukemiaII Aggressive NK leukemia Adult T-cell lymphoma/leukemia (HTLV-1+) Extranodal NK/T-cell lymphoma, nasal type# Enteropathy-like T-cell lymphoma** Hepatosplenic γδ T-cell lymphoma* Subcutaneous panniculitis-like T-cell lymphoma* Mycosis fungoides/Sézary syndrome Anaplastic large cell lymphoma, T/null cell, primary cutaneous type Peripheral T-cell lymphoma, not otherwise characterized Angioimmunoblastic T-cell lymphoma Anaplastic large cell lymphoma, T/null cell, primary systemic type Hodgkin’s Lymphoma (Hodgkin’s Disease) Nodular lymphocyte predominance Hodgkin’s lymphoma Classic Hodgkin’s lymphoma Nodular sclerosis Hodgkin’s lymphoma (grades 1 and 2) Lymphocyte-rich classic Hodgkin’s lymphoma Mixed cellularity Hodgkin’s lymphoma Lymphocyte depletion Hodgkin’s lymphoma † Not described in REAL classification § Includes the so-called Burkitt-like lymphomas ** Formerly known as intestinal T-cell lymphoma # Formerly know as angiocentric lymphoma WHO/REAL Classification of Lymphoid Neoplasms
NHL v HD ? • HD spreads in contiguous fashion from one nodal area to next geographical area • NHL more widespread at presentation • NHL more likely to have disease on both sides of diaphragm • Waldeyers ring involvement suggests NHL • HL predominantly in young people Biopsy with immunohistochemistry is definitive
Histology CD20 expression in DLBCL
Diffuse Large B-cell Lymphoma (high grade lymphoma) • Most common NHL (~35%) • Typically de novo but can arise following transformation • Affects both sexes equally • Median age at diagnosis is 50 years • Can arise in nodal sites and extranodal sites • Highly aggressive • Highly responsive to combination chemotherapy ~ 40% of patients with advanced stage achieving a cure
Staging Lymphoma • Assessment of extent of disease before and after treatment • Indication of prognosis • May dictate nature and intensity of treatment • Investigations: • CT scans • Bone marrow biopsy
Cotswold Classification (modifiedAnn Arbor) staging • Stage I - Involvement of only one lymph node region • Stage II - Two or more lymph node areas involved confined to one side of the diaphragm • Stage III - Involvement of lymph nodes above and below the diaphragm • Stage IV – Multi-focal involvement of an extranodal site • A = No constitutional symptoms • B = Constitutional symptoms present ( 10% weight loss; night sweats; unexplained fever – but not pruritis) • E = Extra-nodal disease at a single site with or without adjacent adenopathy (IE or IIE; by convention IIIE is stage IV) • X = Bulk disease. > 10cm max dimension or >1/3rd widening of mediastinum
Involved areas • Each rectangle corresponds to one nodal area • Count 2 sites if bilateral • Spleen is considered extra nodal site
Staging scans Pre treatment: neck, thorax, abdo, pelvis Interim - if clinical response uncertain or not assessable Post treatment (Follow up) PET scanning now routine pre and post treatment for DLBCL (and hodgkin)
International Prognostic Index( For DLBCL treated with R-CHOP) • Age > 60 • Elevated LDH • Ann Arbor Stage III or IV • ECOG PS ≥ 2 • Number of Extranodal sites > 1 Blood 2006
Management of NHL • Indolent • Watch and wait • Chemo for symptomatic disease • Rituximab based regimes (R-CVP) • Aggressive • Localised (stage 1A) or medically unfit • Radiotherapy • Advanced • Chemo with Rituximab based regimes (R-CHOP) for B cell neoplasms
Side effects of treatment • Acute • Hair loss • Myelosupression (sepsis) • Emesis • Neuropathy • Pulmonary fibrosis • Longer term • Infertility • Hypothyroidism • Secondary malignancy • Myelodysplasia/leukaemia • Breast cancer (esp if radiotherapy before mid 20s) • Lung cancer • Cardiac disease
Late effects of treatment GOALS OF TREATMENT • Risks are increased by combined modality therapy (chemo plus RT) • Risks increased with larger radiation field and with mustine type drugs (MOPP) Can we reduce treatment further for those with early favourable disease? • Prognostic scores • Imaging How do we identify those that need additional treatment to maximise effectiveness? Effective treatment Minimise complications v
Individualising treatment • More aggressive regimes for poor prognosis disease • eg testicular lymphoma, Burkitts, T cell lymphomas • Reducing chemo based on predicted good outcome • Modification for co morbidities eg to encompass more elderly patients
Cancer standards: the MDT • MDT brings together all the professionals who are involved in diagnosis and care • Aims to improve quality of diagnosis and ensure equitable access to best possible care either at local hospital of cancer centre • Members should include cancer experts from specialist centres • Access to trials and research discussed • Holistic issues important • Discussions recorded with plans and outcomes documented: patient offered copy • MDT arrangements subject to peer review
The central purpose of the MDT meeting is to review every new case on a prospective, multi-disciplinary basis, identify missing data and those • investigations requiring further analysis, assign clinical stage, prognostic • scores (IPI, Hasenclever, EORTC) and determine appropriate • management/eligibility for trial entry according to network guidelines.
Amanda starts chemotherapy the following week. Dr White gets a phone call from Dr Black as the school have written to him requesting details of her treatment and when she might be fit to return to work. Dr White understands from Amanda that there will be pressure on her to return as soon as possible and she is worried about paying her mortgage if her sick pay runs out.
Consider the patient’s perspective • Issues affecting cancer patients • Telling family and friends • Work • Childcare • Sexual relationships • Financial • Psychological • Respect individuals privacy and wishes
Sources of support for cancer patients • Nurse and other trained counsellors • Social workers • Written information: BACUP, LRF, Lymphoma association, (internet) • Complimentary therapies