Download
1 / 24
240 likes | 679 Views
Gram Positive Cocci - Staphylococci. DMD 3 rd Semester Dr Ekta Chourasia. GPC Staphylococcus Streptococcus Enterococcus. GNC Neisseria Moraxella. Medically Important Cocci. Gram Positive Cocci (GPC). Staphylococcus (GPCs in clusters) Staphylococcus aureus S. epidermidis

E N D
Gram Positive Cocci - Staphylococci DMD 3rd Semester Dr Ekta Chourasia
GPC Staphylococcus Streptococcus Enterococcus GNC Neisseria Moraxella Medically Important Cocci Micro/DMD/3rd Sem Dr Ekta
Gram Positive Cocci (GPC) Staphylococcus(GPCs in clusters) • Staphylococcus aureus • S. epidermidis • S. saprophyticus Streptococcus(GPCs in chains) • Streptococcus pyogenes (Group A ) • Streptococcus agalactiae (Group B) • Streptococcus pneumoniae (Pneumococcus) • Streptococcus viridans • Enterococcus (Group D) Micro/DMD/3rd Sem Dr Ekta
Staphylococcus 1 Micro/DMD/3rd Sem Dr Ekta
Overview • Main group of medically important gram positive cocci along with streptococci • Infections range from severe to fatal conditions • Difficult to treat, especially those acquired in the hospital • Remarkable ability to acquire antibiotic resistance • Ubiquitous - Part of human flora, inanimate objects Micro/DMD/3rd Sem Dr Ekta
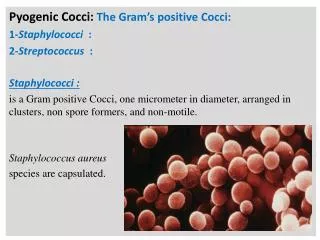
Staphylococci – General features • Gram +ve cocci arranged in grape like cluster • Facultative anaerobes • Produce catalase • Major component of normal flora in humans • Skin • Nose • Mucosal membranes Micro/DMD/3rd Sem Dr Ekta
Clinically Important Species • S. aureus – Coagulase + ve • Most virulent species • Commonest cause of bacterial infections, food poisoning & toxic shock syndrome • Coagulase –ve Staphylococci • S. epidermidis – important cause of prosthetic implant infections • S. saprophyticus – Urinary Tract Infection in young women Micro/DMD/3rd Sem Dr Ekta
Staphylococcus aureus – Important features • Coagulase positive • Beta hemolytic colonies on BA • Produces golden yellow pigment • Highly resistant bacteria • Can grow in the presence of 10 – 15% NaCl Micro/DMD/3rd Sem Dr Ekta
Virulence Factors • Toxins – cytolytic & superantigen exotoxins • Enzymes & • Cell associated polymers and surface proteins Micro/DMD/3rd Sem Dr Ekta
1. Toxins • Cytolytic toxins • Haemolysins- lyse RBCs of various animal species • Leucocidins - kills leucocytes • Superantigens • Enterotoxin A to E - Food poisoning • Toxic shock syndrome toxin (TSST/ Enterotoxin F) – Toxic Shock Syndrome: rash, desquamation, multi organ failure • Epidermolytic ( Exfoliative ) toxin A & B – SSSS: Staphylococcal scalded skin syndrome (epidermal splitting & exfoliation) Micro/DMD/3rd Sem Dr Ekta
2. Extracellular enzymes • Catalase – enhance their survival in phagocytes by inactivating toxic H2O2 & free radicals released after the ingestion of staphylococci. • Coagulase - Clots plasma, responsible for ‘tube coagulase test’, confirmatory test for S.aureus • Hyaluronidase - Breaks down hyaluronic acid (connective tissue): initiation & spread of infection • Fibrinolysin (Staphylokinase) - Lyses fibrin clots: spread of infection • Nuclease - hydrolyses DNA • Lipase – Lipolytic: infection of skin & subcutaneous tissue Micro/DMD/3rd Sem Dr Ekta
3. Surface proteins • Protein A - Antiphagocytic • Clumping factor - bound coagulase, responsible for ‘slide coagulase test’, screening test for S.aureus Micro/DMD/3rd Sem Dr Ekta
Pathogenicity of S. aureus • Cutaneous infections – • Folliculitis (boils), furuncle, burns and wounds • Deep infections – • Osteomyelitis (commonest cause), abscesses, pneumonia, endocarditis, septicemia • Nosocomial infections – • Surgical wound infection • Catheter associated bacteremia Abscess Folliculitis Micro/DMD/3rd Sem Dr Ekta
Pathogenicity of S. aureus • Toxin mediated infections – • Toxic Shock Syndrome (TSS) : Caused by TSST-1 (Enterotoxin F) – mostly in females, fatal multisystem disease • Staphylococcal scalded skin syndrome (SSSS) : Exfoliative skin disease – damage to desmosomes - outer layer of epidermis separates out from the underlying tissues • Food poisoning (in 1-8hr, vomiting, diarrhea, nausea, self limited ) Toxic shock syndrome SSSS Micro/DMD/3rd Sem Dr Ekta
Pathogenicity (Staphylococcal diseases) Micro/DMD/3rd Sem Dr Ekta
Lab diagnosis – S. aureus • Specimens: wound swab, pus, blood, feces • Microscopy: Gram stain - GPC in clusters • Culture • Blood Agar : beta hemolysis • Nutrient Agar : golden yellow pigment • Mannitol salt agar – selective media • Catalase positive • Coagulase positive Micro/DMD/3rd Sem Dr Ekta
Coagulase Test Micro/DMD/3rd Sem Dr Ekta
Staphylococcus epidermidis Major component of skin flora Nosocomial infections: device/ implant associated infections - shunts, catheters, artificial heart valves / joints, pacemaker BA: Non - hemolytic Identification Coagulase negative Prosthetic valve endocarditis Micro/DMD/3rd Sem Dr Ekta
Drug Resistance in Staphylococci & MRSA • First developed resistance against Penicillin • Resistance to penicillin is mainly attributed to the production of enzyme, Penicillinase (beta-lactamase) • To combat resistance due to penicillinase, Methicillin was developed & now methicillin resistant strains have evolved – MRSA Micro/DMD/3rd Sem Dr Ekta
MRSA(Methicillin Resistant S. aureus) • Important cause of Nosocomial infections • post surgical wound infections • blood stream infections • ventilator associated pneumonia • Patients with open wounds, invasive devices and weakened immune systems are at greater risk for infection • Person to person spread – mainly from carriers (hospital staff, visitors), 25-30% carry in their nose. By contact with • colonized or infected patients • colonized or infected body sites of the personnel themselves, • devices, items, or environmental surfaces contaminated with body fluids containing MRSA. Micro/DMD/3rd Sem Dr Ekta
MRSA(Methicillin Resistant S. aureus) • Difficult to treat • Prevention and infection-control strategies • Screening of staphylococcal carriers among hospital staff • Treatment of carriers with mupirocin, hexachlorophene • Proper sanitary procedures – surface sanitation, hand washing (alcohol gels), personal protective measures • Isolation of patients with open staphylococcal lesions * However carrier status prevents complete control • Treatment of MRSA infection - Glycopeptides • Vancomycin • Teicoplanin Micro/DMD/3rd Sem Dr Ekta
Overview of Medically Important Staphylococci Micro/DMD/3rd Sem Dr Ekta
In clusters (grapes like) or short chains Catalase + ve Facultative anaerobes Grows on ordinary medium Major components of normal flora – skin, nose & mucosa Produces localized infections Resistant to drying, Penicillin In chains or in pairs Catalase -ve Obligate & facultative anaerobes, grows in 5-10% CO2 Fastidious – requires enriched medium like BA Normal flora in throat, colon, female genital tract Infections tend to spread Delicate organism, sensitive to penicillin Staphylococci v/s Streptococci Micro/DMD/3rd Sem Dr Ekta