Download
1 / 56
570 likes | 703 Views
Oxygen Therapy. Mark Carpenter ICU Consultant CHS Jan 2016. Quiz. High-flow oxygen (non-rebreathe mask) Controlled oxygen therapy (24% etc) NIV on respiratory ward Call ICU for consideration of ventilation No need for Oxygen therapy.

E N D
Oxygen Therapy Mark Carpenter ICU Consultant CHS Jan 2016
Quiz • High-flow oxygen (non-rebreathe mask) • Controlled oxygen therapy (24% etc) • NIV on respiratory ward • Call ICU for consideration of ventilation • No need for Oxygen therapy
Lifelong smoker admitted with cough: SpO2 82%, pH 7.4, pCO2 8.0 pO2 5.4 • High-flow oxygen (non-rebreathe mask) • Controlled oxygen therapy (24% etc) • NIV on respiratory ward • Call ICU for consideration of ventilation • No need for Oxygen therapy
Post Cardiac Arrest Patient: cold peripheries, BP 120/70, No ABG, RR 28/min • High-flow oxygen (non-rebreathe mask) • Controlled oxygen therapy (24% etc) • NIV on respiratory ward • Call ICU for consideration of ventilation • No need for Oxygen therapy
Lifelong smoker admitted with cough: SpO2 90%, pH 7.25, pCO2 9.0 pO2 7.0 • High-flow oxygen (non-rebreathe mask) • Controlled oxygen therapy (24% etc) • NIV on respiratory ward • Call ICU for consideration of ventilation • No need for Oxygen therapy
Young asthmatic, SpO2 84%, RR 28/min, pH 7.44, pCO2 2.0, pO2 6.2 • High-flow oxygen (non-rebreathe mask) • Controlled oxygen therapy (24% etc) • NIV on respiratory ward • Call ICU for consideration of ventilation • No need for Oxygen therapy
Patient on Surgical ward having iv morphine PCA: Sats 95% on Air • High-flow oxygen (non-rebreathe mask) • Controlled oxygen therapy (24% etc) • NIV on respiratory ward • Call ICU for consideration of ventilation • No need for Oxygen therapy
Patient admitted with Pneumonia (frail and elderly: pO2 12, pCO2 8.0, pH7.1, RR 32/min • High-flow oxygen (non-rebreathe mask) • Controlled oxygen therapy (24% etc) • NIV on respiratory ward • Call ICU for consideration of ventilation • No need for Oxygen therapy
Oxygen - there is a problem Published audits have shown • Doctors and nurses have a poor understanding of how oxygen should be used • Oxygen is often given without any prescription • If there is a prescription, it is unusual for the patient to receive what is specified on the prescription
Oxygen - there was a disagreement • Chest Physicians • Intensivists • Emergency Medicine / A&E clinicians • Ambulance teams
Assessment/Measurement of Hypoxaemia CYANOSIS - Often not recognised, - Absent with anaemia BLOOD GASES - PaO2 OXYGEN SATURATION - Easily measured - Widely available
Prescribing by target oxygen saturationBasis of the BTS guidelineKeep it normal/near-normal for all patients except pre-defined groups who are at risk from hypercapnic respiratory failure
Normal Range for Oxygen saturation Normal range for healthy young adults is approximately 96-98%(Crapo AJRCCM, 1999;160:1525) Is the oxygen saturation lower in elderly people? Previous literature suggested a gradual fall with advancing age However, a recent Salford/Southend audit of 320 stable adults aged >70 found Mean SpO2 96.7% 2SD range 93.1-100%
What is a “normal” nocturnal oxygen saturation? • Healthy subjects in all age groups routinely desaturate to an average nadir of 90.4% during the night (SD 3.1%) Gries RE et al Chest 1996; 110: 1489-92 *Therefore, be cautious in interpreting a single oximetry measurement from a sleeping patient. Watch the oximeter for a few minutes if in any doubt (if the patient is othewise stable) as normal overnight dips are of short duration.
Clinical features of Hypoxaemia Often non-specific Depends if onset is chronic or acute • Altered mental state • Dyspnoea, cyanosis, tachypnoea, arrhythmias, coma • Hyperventilation when PaO2 <5.3kPa (saturation <72%) • Loss of consciousness ~ 4.3 kPa • Death approximately 2.7 kPa
Effects of sudden hypoxia(e.g Removal of oxygen mask at altitude or in a pressure chamber) • Mean SaO2 of airline passengers falls from 97% to 93% (average nadir 88.6%) with no apparent effects • Impaired mental function; Mean onset at SaO2 64% No evidence of impairment above 84% saturation • Loss of consciousness at mean saturation of 56% Note absence of breathlessness at rest with sudden hypoxia but no disease Also note that oxygen has no effect on the sensation of breathlessness in patients who are not hypoxaemic Akero A et al Eur Respir J. 2005 ;25:725-30 Cottrell JJ et al Aviat Space Environ Med. 1995 ;66:126-30 Hoffman C, et al. Am J Physiol 1946, 145, 685-692
What happens at 9,000 metres (approximately 29,000 feet) – it depends Atmospheric pO2 6.2 kPa (< 1/3 sea level pO2) PaO2 ~3.3 kPa Arterial Oxygen Saturation ~70% SUDDEN ACCLIMATISATION Passengers unconscious in <60 seconds if depressurised Everest has been climbed without oxygen
Aims of emergency oxygen therapy • To correct or prevent potentially harmful hypoxaemia • To alleviate breathlessness (only if hypoxaemic) • Oxygen has no effect on breathlessness if the oxygen saturation is normal
But some patients are at risk of CO2 retention and acidosis if given high dose oxygen • Chronic hypoxic lung disease • COPD • Severe Chronic Asthma • Bronchiectasis / CF • Chest wall disease • Kyphoscoliosis • Thoracoplasty • Neuromuscular disease • Obesity hypoventilation
Oxygen therapy is only one element of resuscitation of a critically ill patient The oxygen carrying power of blood may be increased by • Enhancing circulating volume • Correcting severe anaemia • Enhancing cardiac output • Safeguarding the airway • Avoiding/Reversing Respiratory Depressants • Increasing Fraction of Inspired Oxygen (FIO2) • Establish the reason for Hypoxia and treat the underlying cause (e.g Bronchospasm, LVF etc) • Patient may need, CPAP or NIV or Invasive ventilation
Exposure to high concentrations of oxygenmay be harmful • Absorption Atelectasis even at FIO2 30-50% • Intrapulmonary shunting • Post-operative hypoxaemia • Risk to COPD patients • Coronary vasoconstriction • Increased Systemic Vascular Resistance • Reduced Cardiac Index • Possible reperfusion injury post MI • Worsens systolic myocardial performance • Oxygen therapy INCREASED mortality in non-hypoxic patients with mild-moderate stroke RECOMMENDATION – This guideline recommends an upper limit of 98% for most patients. This is a combination of what is normal and safe Harten JM et al J Cardiothoracic Vasc Anaesth 2005; 19: 173-5 Kaneda T et al. Jpn Circ J 2001; 213-8 Frobert O et al. Cardiovasc Ultrasound 2004; 2: 22 Haque WA et al. J Am Coll Cardiol 1996; 2: 353-7 Thomaon aj ET AL. BMJ 2002; 1406-7 Ronning OM et al. Stroke 1999; 30
pO2 above 6.7 kPa or 50 mm Hg in acute COPD will prevent death (SpO2 above about 85%) OxyHaemoglobin Dissociation Curve SaO2 mmHg PaO2 What is a safe lower Oxygen level in acute COPD? This guideline recommends a minimum oxygen saturation of 88% for most patients with COPD Murphy R, Driscoll P, O’Driscoll R Emerg Med J 2001; 18:333-9
47% of 982 patients with exacerbation of COPD were hypercapnic on arrival in hospital 20% had Respiratory Acidosis (pH < 7.35) 5% had pH < 7.25 (and were likely to need ICU care) Most hypercapnic patients with pO2 > 10 kPa were acidotic (equivalent to oxygen saturation of above ~ 92%) i.e. had been given too much oxygen RECOMMENDATION: Keep PaO2 below 10 kPa and SpO2 < 92% in acute COPD What is a safe higher oxygen level in acute COPD Plant et al Thorax 2000; 55:550
Fallacies regarding Oxygen Therapy“Routine administration of supplemental oxygen is useful, harmless and clinically indicated” • Renders pulse oximetry worthless as a measure of ventilation • May prevent early diagnosis and specific treatment of hypoventilation This guideline only recommends supplemental oxygen when the patients oximetry is below the target range John B Downs MD Respiratory care 2003;48:611-20
Fallacies regarding Oxygen Therapy“High FIO2 is Protective for individuals at risk of hypoxaemia” Little increase in oxygen-carrying capacity No known benefit in maintaining saturation above 90% This guideline recommends an upper limit of 98% for patients not at risk of acute hypercapnic respiratory failure John B Downs MD Respiratory Care 2003; 48:611-20
Target Saturation Scheme • O2 prescribed by target saturation (like an Insulin “BM sliding-scale chart”) • Oxygen delivery device and flow administered and changed if necessary to keep the SpO2 in the target range • Target oxygen saturation prescription integrated into patient drug chart and monitoring
Recommended target saturations The target ranges are a consensus agreement by the guidelines group and the endorsing colleges and societies Rationale for the target saturations is combination of what is normal and what is safe Most patients 94 - 98% Risk of hypercapnic respiratory failure88 – 92%* *Or patient specific saturation on Alert Card
Safeguarding patients at risk of type 2 respiratory failure • Lower target saturation range for these patients (88-92%) • Education of patients and health care workers • Use of controlled oxygen via Venturi masks • Use of oxygen alert cards • Issue of personal Venturi masks to high-risk patients
Oxygen Alert Cards and 24% masks (recommended in guideline) can avoid hypercapnic respiratory failure associated with high flow oxygen masks • Oxygen alert card (and a 24% Venturi mask) given to patients admitted with hypercapnic acidosis with a PO2 > 10kPa. • Patients instructed to show these to ambulance and A&E staff. After introduction of alert cards • Use of 24% oxygen: 63% in Ambulance 94% in A&E Gooptu B, Ward L, Davison A et al. Oxygen alert cards and controlled oxygen masks: Emerg Med J 2006; 23:636-8
OXYGEN ALERT CARD Name: ______________________________ I am at risk of type II respiratory failure with a raised CO2 level. Please use my % Venturi mask to achieve an oxygen saturation of _____ % to _____ % during exacerbations Use compressed air to drive nebulisers (with nasal oxygen at 2 l/min). If compressed air not available, limit oxygen-driven nebulisers to 6 minutes.
High Concentration Reservoir Mask • Non re-breathing Reservoir Mask. • Critical illness / Trauma patients. • Post-cardiac or respiratory arrest. • Delivers O2 concentrations between 60 & 80% or above • Effective for short term treatment.
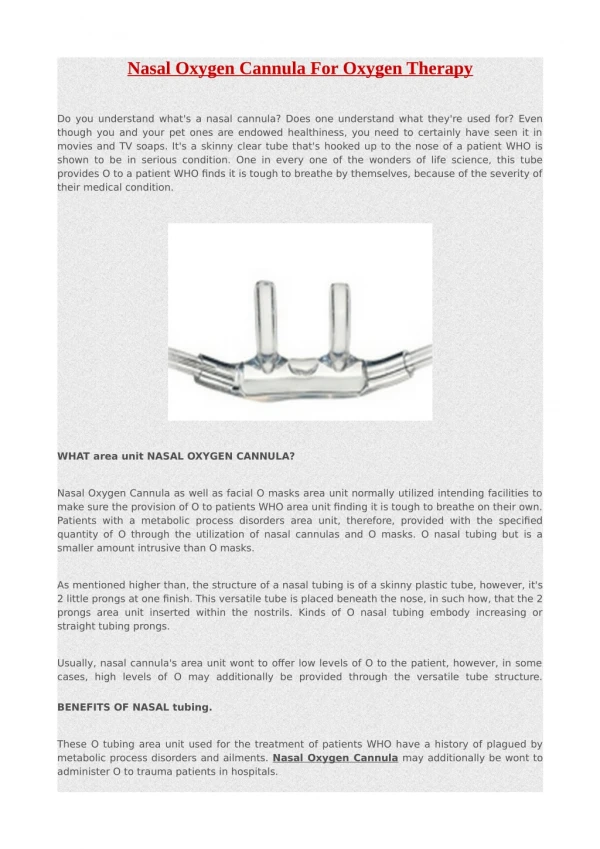
Nasal Cannulae • Recommended in the Guideline as suitable for most patients with both type I and II respiratory failure. • 2-6L/min gives approx 24-50% FIO2 • FIO2 depends on oxygen flow rate and patient’s minute volume and inspiratory flow and pattern of breathing. • Comfortable and easily tolerated • No re-breathing • Low cost product • Preferred by patients (Vs simple mask)
Simple face mask(Medium concentration, variable performance) • Used for patients with type I respiratory failure. • Delivers variable O2 concentration between 35% & 60%. • Low cost product. • Flow 5-10 L/min Flow must be at least 5 L/min to avoid CO2 build up and resistance to breathing (although packaging says 2-10L)
Venturi or Fixed Performance Masks Aim to deliver constant oxygen concentration within and between breaths. VENTIMASKS 24-40% operate satisfactorily A 60% mask gives 50% FIO2 With TACHYPNOEA (RR >30/min) the oxygen supply should be increased by 50% Increasing flow does not increase oxygen concentration
Operation of Venturi valve Air O2 + Air O2 Air For 24% Venturi mask, the typical oxygen flow of 2 l/min gives a total gas flow of 51 l/minFor 28% Venturi mask, 4 l/min oxygen flow, gives a total gas flow of 44 l/min(Table 10.2)
Many patients need high-dose oxygen to normalize saturation • Severe Pneumonia • Severe LVF • Major Trauma • Sepsis and Shock • Major atelectasis • Pulmonary Embolism • Lung Fibrosis • Etc etc etc
Oxygen prescription for acutely hypoxaemic patients in hospital Yes Is the patient critically ill or in a peri-arrest condition? Commence treatment with reservoir mask or bag-valve mask No Is this patient at risk of hypercapnic respiratory failure (Type 2 Respiratory Failure)? YES Target saturation is 88-92 % (or level on alert card)whilst awaiting blood gas results. NO Aim for SpO2 94-98%
Risk of CO2 Retention Start 28% or 24% oxygen and obtain ABGs Reduce FIO2 if SpO2 >92% or above the range stated on alert card. No known Risk of CO2 Retention SpO2 < 94% on air or oxygen Or needing oxygen to achieve above targets Yes: Commence oxygen as per tables 2 or 4 and CHECK ABGs No pH <7.35 and PCO2 > 6.0 (Respiratory Acidosis) or patient tiring PCO2< 6.0 (Normal or low) PCO2 >6.0 Or respiratory deterioration (see box in chart 2) Monitor SpO2. Oxygen not required unless SpO2 falls below target range pH > 7.35 and PaCO2 >6kPa (Hypercapnia) Seek immediate senior review Consider NIV or invasive ventilation Treat with the lowest strength Venturi mask that will keep SpO2 between 88-92% Seek immediate senior review Consider invasive ventilation Treat appropriately aiming to keep SpO2 94-98%** Repeat ABG in 30-60 min for all patients at risk of type 2 Respiratory Failure Treat with lowest FiO2 to keep SpO288-92% via Venturi mask pending senior medical advice or NIV or ICU admission Repeat ABG’s at 30-60 mins If Respiratory Acidosis ( pH <7.35 & PCO2>6.0) Seek immediate senior review, consider NIV/ICU. Consider reducing FiO2 if PO2 > 8.0 kPa Treat urgently. Aim for SpO2 of 94-98% until immediate senior review. Also consider COPD needing SpO2 88-92% Treat appropriately aiming to keep SpO2 94-98%
Risk of CO2 Retention Start 28% or 24% oxygen and obtain ABGs Reduce FIO2 if SpO2 >92% or above the range stated on alert card. No known Risk of CO2 Retention SpO2 < 94% on air or oxygen Or needing oxygen to achieve above targets Get Help Quick About to arrest Don’t treat the gas, what is the patient like?? Yes: Commence oxygen as per tables 2 or 4 and CHECK ABGs No pH <7.35 and PCO2 > 6.0 (Respiratory Acidosis) or patient tiring PCO2< 6.0 (Normal or low) PCO2 >6.0 Or respiratory deterioration (see box in chart 2) Monitor SpO2. Oxygen not required unless SpO2 falls below target range pH > 7.35 and PaCO2 >6kPa (Hypercapnia) Seek immediate senior review Consider NIV or invasive ventilation Treat with the lowest strength Venturi mask that will keep SpO2 between 88-92% Seek immediate senior review Consider invasive ventilation Treat appropriately aiming to keep SpO2 94-98%** Repeat ABG in 30-60 min for all patients at risk of type 2 Respiratory Failure Treat with lowest FiO2 to keep SpO288-92% via Venturi mask pending senior medical advice or NIV or ICU admission Repeat ABG’s at 30-60 mins If Respiratory Acidosis ( pH <7.35 & PCO2>6.0) Seek immediate senior review, consider NIV/ICU. Consider reducing FiO2 if PO2 > 8.0 kPa Treat urgently. Aim for SpO2 of 94-98% until immediate senior review. Also consider COPD needing SpO2 88-92% Treat appropriately aiming to keep SpO2 94-98%
Risk of CO2 Retention Start 28% or 24% oxygen and obtain ABGs Reduce FIO2 if SpO2 >92% or above the range stated on alert card. No known Risk of CO2 Retention SpO2 < 94% on air or oxygen Or needing oxygen to achieve above targets Get Help Quick Is this really COPD, in which case NIV on ward OK, or is it failing type 1 failure?? Don’t treat the gas, what is the patient like?? Yes: Commence oxygen as per tables 2 or 4 and CHECK ABGs No pH <7.35 and PCO2 > 6.0 (Respiratory Acidosis) or patient tiring PCO2< 6.0 (Normal or low) PCO2 >6.0 Or respiratory deterioration (see box in chart 2) Monitor SpO2. Oxygen not required unless SpO2 falls below target range pH > 7.35 and PaCO2 >6kPa (Hypercapnia) Seek immediate senior review Consider NIV or invasive ventilation Treat with the lowest strength Venturi mask that will keep SpO2 between 88-92% Seek immediate senior review Consider invasive ventilation Treat appropriately aiming to keep SpO2 94-98%** Repeat ABG in 30-60 min for all patients at risk of type 2 Respiratory Failure Treat with lowest FiO2 to keep SpO288-92% via Venturi mask pending senior medical advice or NIV or ICU admission Repeat ABG’s at 30-60 mins If Respiratory Acidosis ( pH <7.35 & PCO2>6.0) Seek immediate senior review, consider NIV/ICU. Consider reducing FiO2 if PO2 > 8.0 kPa Treat urgently. Aim for SpO2 of 94-98% until immediate senior review. Also consider COPD needing SpO2 88-92% Treat appropriately aiming to keep SpO2 94-98%
Risk of CO2 Retention Start 28% or 24% oxygen and obtain ABGs Reduce FIO2 if SpO2 >92% or above the range stated on alert card. No known Risk of CO2 Retention SpO2 < 94% on air or oxygen Or needing oxygen to achieve above targets Type 1 resp failure Treat cause and hypoxaemia with O2 Don’t treat the gas, what is the patient like?? Beware a rise in CO2 Yes: Commence oxygen as per tables 2 or 4 and CHECK ABGs No pH <7.35 and PCO2 > 6.0 (Respiratory Acidosis) or patient tiring PCO2< 6.0 (Normal or low) PCO2 >6.0 Or respiratory deterioration (see box in chart 2) Monitor SpO2. Oxygen not required unless SpO2 falls below target range pH > 7.35 and PaCO2 >6kPa (Hypercapnia) Seek immediate senior review Consider NIV or invasive ventilation Treat with the lowest strength Venturi mask that will keep SpO2 between 88-92% Seek immediate senior review Consider invasive ventilation Treat appropriately aiming to keep SpO2 94-98%** Repeat ABG in 30-60 min for all patients at risk of type 2 Respiratory Failure Treat with lowest FiO2 to keep SpO288-92% via Venturi mask pending senior medical advice or NIV or ICU admission Repeat ABG’s at 30-60 mins If Respiratory Acidosis ( pH <7.35 & PCO2>6.0) Seek immediate senior review, consider NIV/ICU. Consider reducing FiO2 if PO2 > 8.0 kPa Treat urgently. Aim for SpO2 of 94-98% until immediate senior review. Also consider COPD needing SpO2 88-92% Treat appropriately aiming to keep SpO2 94-98%
Any increase in FIO2 must be followed by repeat ABGs in 1 hour (or sooner if conscious level deteriorates)If pH is < 7.35 ([H+] > 45 nmol/L) with normal or low PaCO2, investigate and treat for metabolic acidosis and keep SpO2 94-98% Patients previously requiring NIV or IPPV should have a target range of 88-92% even if the initial paCO2 is normal
Lifelong smoker admitted with cough: SpO2 82%, pH 7.4, pCO2 8.0 pO2 5.4 • High-flow oxygen (non-rebreathe mask) • Controlled oxygen therapy (24% etc) • NIV on respiratory ward • Call ICU for consideration of ventilation • No need for Oxygen therapy