Download
1 / 82
830 likes | 907 Views
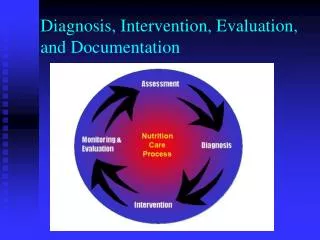
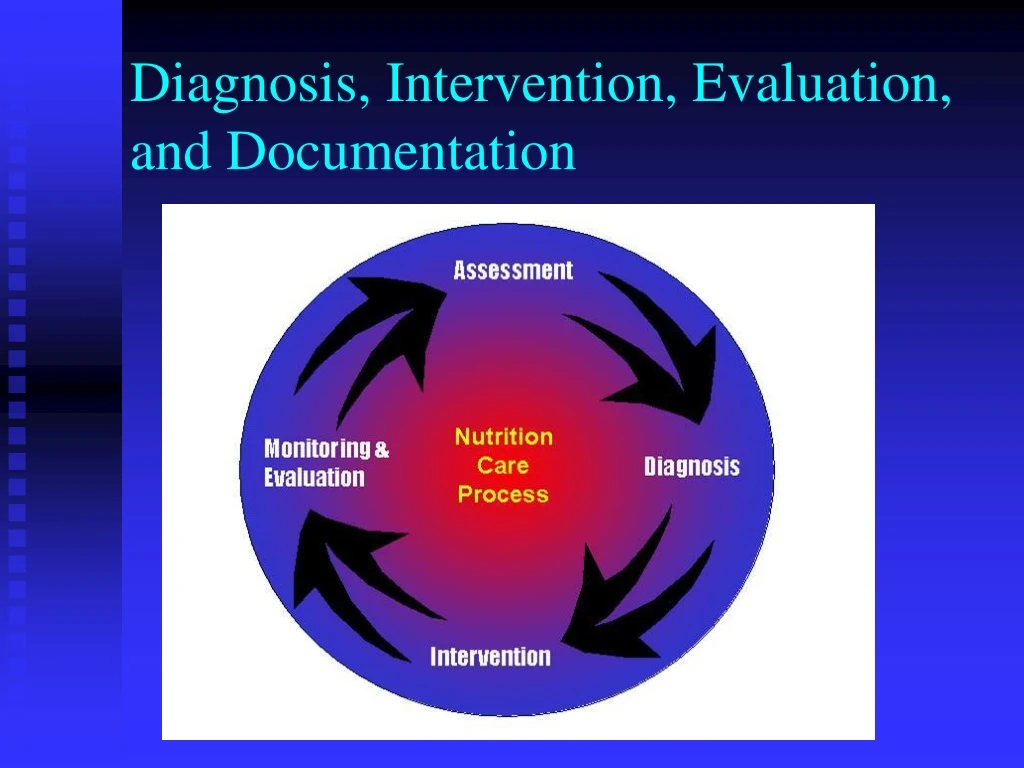
Diagnosis, Intervention, Evaluation, and Documentation. Ø. ADA NUTRITION CARE PROCESS. AND MODEL. Screening. & Referral. System. Ø. Identify risk factors. Ø. Use appropriate tools. and methods. Ø. Involve. interdisciplinary. collaboration. Nutrition Diagnosis. Ø.

E N D
Ø ADA NUTRITION CARE PROCESS AND MODEL Screening & Referral System Ø Identify risk factors Ø Use appropriate tools and methods Ø Involve interdisciplinary collaboration Nutrition Diagnosis Ø Identify and label problem Nutrition Assessment Ø Determine cause/contributing risk Ø Obtain/collect timely and factors appropriate data Ø Cluster signs and symptoms/ Ø Analyze/interpret with defining characteristics evidence - based standards Ø Document Document Relationship Between Patient/Client/Group Nutrition Intervention Dietetics & Ø Plan nutrition intervention · Professional Formulate goals and determine a plan of action Implement the nutrition intervention Ø · Care is delivered and actions Nutrition Monitoring and - are carried out Evaluation Ø Documen t Ø Monitor progress Ø Measure outcome indicators Ø Evaluate outcomes Ø Document Outcomes Management Sys tem Ø Monitor the success of the Nutrition Care Process implementation Ø Evaluate the impact with aggregate data Ø Identify and analyze causes of less than optimal performance and outcomes Ø Refine the use of the Nutrition Care Process
Nutrition Assessment Leads to Nutrition Diagnosis • Nutrition Assessment • Nutrition Diagnosis • Nutrition Intervention • Nutrition Monitoring and Evaluation
PES Statement • Problem: nutrition diagnosis label • Etiology: the focus of the intervention • Signs and symptoms: change when nutrition problems are successfully treated; the focus of monitoring and evaluation
Problem (Diagnostic Label) Falls into three general domains: • Intake (NI) • Excessive or Inadequate intake compared to requirements • Clinical (NC) • Medical or physical conditions that are outside normal • Behavioral/environmental (NB) • Knowledge, attitudes, beliefs, physical environment, access to food, food safety
Etiology • Etiology (Cause/Contributing Factors) • Related factors that contribute to problem • Identifies cause of the problem • Helps determine whether nutrition intervention will improve problem • Linked to problem by words “related to” (RT) • Note: etiology may not always be clear
Etiology • Etiology (Cause/Contributing Factors) • Excessive energy intake (problem) “related to” regular consumption of large portions of high-fat meals (etiology)… • Swallowing difficulty (problem) RT recent stroke (etiology)… • Involuntary wt gain RT decrease in exercise…
Diagnostic Labels Can Be Problems or Etiologies • Inadequate energy intake (NI-1.4) related to food-nutrition knowledge deficit (NB-1.1) • Food-nutrition knowledge deficit (NB-1.1) related to lack of previous nutrition education • Involuntary weight loss (NC-3.2) related to inadequate energy intake (NI-1.4) • Inadequate oral food-beverage intake (NI-2.1) related to swallowing difficulty (NC-1.1)
Signs and Symptoms • Signs/Symptoms (Defining characteristics) • Evidence that problem exists • Linked to etiology by words “as evidenced by” • Evaluation and monitoring of effectiveness of intervention is done by reviewing signs and symptoms
Nutrition Dx with S/S • Excessive energy intake (NI-1.5) (P) • “related to” regular consumption of large portions of high-fat meals (E) • “as evidenced by” diet history & 12 lb wt gain over last 18 mo (Signs)
Nutrition Assessment Identifies Etiology and S/S • Problem: excessive energy intake • Etiology: reviewing the diet history, we learn that • Patient eats in fast food restaurants 2x day • Patient supersizes portions because it’s a bargain • Patient has only 15 minutes for lunch
Etiology Guides Intervention! • The clinician determines what the intervention is by looking at the root cause of the nutrition problem. • If the cause of excessive energy intake is eating frequently in fast food restaurants, how would you intervene?
PES Statements • Excessive fat intake (NI-5.6.2) related to high intake of fried foods and bakery goods as evidenced by diet history and hyperlipidemia • Excessive energy intake (NI-1.5) related to high intake of fried foods and snack items as evidenced by diet history and BMI • Food/nutrition related knowledge deficit (NB-1.1) related to lack of education on cholesterol lowering diet as evidenced by history and patient self-report
Nutrition Diagnosis Statement Should Be • Clear, concise • Specific • Related to one problem • Accurate – related to one etiology • Based on reliable, accurate assessment data
Evaluating Your PES Statement • There are no right or wrong PES statements • But some are better than others
Evaluating Your PES Statement • Can the RD resolve or improve the nutrition diagnosis? • Can your intervention address the etiology and thus resolve it or improve the problem? • Or can your intervention address the signs and symptoms?
Evaluating Your PES Statement • Ex: Inadequate energy intake related to decreased taste perception as evidenced by diet history, medical dx and weight loss of 10 lb. during cancer tx • Cannot treat the etiology (decreased taste perception) but can treat S&S by recommending foods with stronger flavors
Evaluating Your PES Statement • Altered nutrition-related labs related to GI bleed as evidenced by medical hx and decreased hgb/hct in medical record • Labs likely won’t improve until GI bleed is addressed; the etiology is not a nutritional deficit • CAN address inadequate intake of iron, copper, B12, protein, etc.
Evaluating Your PES Statement • When all things are equal and there is a choice between two nutrition diagnoses from different domains, consider the Intake domain diagnosis as the one more specific to the role of the RD • Instead of Altered nutrition-related labs related to GI bleed as evidenced by medical hx and decreased hgb/hct in medical record • Consider Inadequate intake of iron (NI-5.10.1) related to increased needs due to GI bleed as evidenced by medical history, blood count, diet history, and serum ferritin
Evaluating Your PES Statement • Will measuring the signs and symptoms tell you if the problem is resolved or improved? • Ex: If nutrition dx is excessive energy intake, can do another diet history at next visit and see if intake has changed; can also check weight
NCP Example: Long Term Care • 85 y.o. resident of LTC facility has lost >10% weight in the last 6 months • Medical workup negative • Oral supplement is ordered but patient continues to lose weight • Nutrition professional is consulted for enteral feeding recommendations
NCP Example: LTC • On assessment, it is found that patient’s teeth no longer fit and she cannot chew regular meats and vegetables; patient is storing oral supplement in drawer as she worries about the cost
NCP Example: LTC • Diagnosis: Inadequate energy intake (NI-1.4) related to poorly fitting dentures and hoarding of oral supplement as evidenced by observation and pt interview
Etiology Guides Intervention • Intervention: Nutrition professional orders dental consult (RC-1.3) to reline dentures and chopped diet (ND-1.2); puts resident on Medpass supplement (ND-3.1.1)
ADA’s Nutrition Care Process Steps • Nutrition Assessment • Nutrition Diagnosis • Nutrition Intervention • Nutrition Monitoring and Evaluation
Nutrition Intervention • Should be targeted at etiology • If not etiology, then signs and symptoms
Nutrition Interventions Four categories of nutrition interventions: • Food and/or nutrient delivery (ND) • Nutrition education (E) • Nutrition counseling (C) • Coordination of nutrition care (RC)
Food and/or Nutrient Delivery • Meals and snacks (ND-1) • Enteral/parenteral nutrition (ND-2) • Medical food supplements (ND-3.1) • Vitamin and mineral supplement (ND-3.2) • Bioactive substance supplement (ND-3.3) • Feeding assistance (ND-4) • Feeding environment (ND-5) • Nutrition-related medication management (ND-6)
Nutrition Education (E) • Initial/brief nutrition education (E-1) • E.g. survival skills on discharge • Comprehensive nutrition education (E-2) • Purpose • Recommended modifications • Result interpretation • Other Note: Education is appropriate for food and nutrition-related knowledge deficit. If the client knows the content, more education probably won’t help
Nutrition Counseling (C) • Theory or approach • Strategies • Phase
Nutrition Counseling: Theory or Approach The theories or models used to design and implement an intervention; provide a research-based rationale for designing and tailoring nutrition interventions • Cognitive-behavioral therapy (C-1.2) • Health belief model (C-1.3) • Social learning theory (C-1.4) • Transtheoretical Model/Stages of Change (C-1.5) • Other (C-1.6)
Motivational interviewing (C-2.1) Goal setting (C-2.2) Self-monitoring (C-2.3) Problem solving (C-2.4) Social support (C-2.5) Stress management (C-2.6) Stimulus control (C-2.7) Cognitive restructuring (C-2.8) Relapse prevention (C-2.9) Rewards/contingency mgt (C-2.10) Other Nutrition Counseling: Strategies* *Selectively applied evidence-based method or plan of action designed to achieve a particular goal
Coordination of Care (RC) • Coordination of other care during nutrition care (RC-1) • Team meeting • Referral to RD • Collaboration with other providers • Referral to community agencies/programs • Discharge and transfer of nutrition care to new setting/provider (RC-2) • Collaboration • Referral to community agencies/programs
ADA’s Nutrition Care Process Steps • Nutrition Assessment • Nutrition Diagnosis • Nutrition Intervention • Nutrition Monitoring and Evaluation
Nutrition Monitoring and Evaluation • Monitor progress and determine if goals are met • Identifies patient/client outcomes relevant to the nutrition diagnosis and intervention plans and goals • Measure and compare to client’s previous status, nutrition goals, or reference standards
Nutrition Outcomes – 4 Categories • Nutrition-Related Behavioral and Environmental Outcomes (BE)—Nutrition-related knowledge, behavior, access, and ability that impact food and nutrient intake • Food and Nutrient Intake Outcomes (FI)—Food and/or nutrient intake from all sources • Nutrition-Related Physical Signs and Symptom Outcomes (S)—Anthropomorphic, biochemical, and physical exam parameters • Nutrition-Related Patient/client centered Outcomes (PC)—perception of patient/client’s nutrition intervention and its impact
Nutrition-Related Behavioral and Environmental Outcomes (BE) • Knowledge/beliefs (1) • Behavior (2) • Access (3) • Physical activity and function (4)
Behavior-Environmental Outcomes Domain: Beliefs and Attitudes (BE-1.1) Definition: beliefs/attitudes about and/or readiness to change food, nutrition, or nutrition-related behaviors Potential indicators (BE-1.1) • Readiness to change • Perceived consequences of change • Perceived costs versus benefits of change • Perceived risk • Outcome expectancy • Conflict with patient/family value system • Self efficacy
Beliefs and Attitudes (BE-1.1) Measurement methods or data sources • Patient self-report, client/patient assessment questionnaire or interview Typically used to monitor and evaluate change in the following domains of nutrition intervention: • Nutrition education, nutrition counseling
Beliefs and Attitudes (BE-1.1) Typically used to monitor and evaluate change in the following nutrition diagnoses • Harmful beliefs/attitudes about food- or nutrition-related topics • Not ready for diet/lifestyle change • Inability to manage self-care • Excess or inadequate oral food/beverage, energy, macronutrient, micronutrient, or bioactive substance intake • Imbalance of nutrients • Inappropriate fat foods
Beliefs and Attitudes (BE-1.1) Typically used to monitor/evaluate change in the following nutrition diagnoses (cont) • Inappropriate intake of amino acids • Underweight • Overweight/obesity • Disordered eating pattern • Physical inactivity • Excess exercise
Behavior-Environmental Outcomes Domain: Food and Nutrition Knowledge (BE-1.2) Definition: Level of knowledge about food, nutrition and health, or nutrition-related information and guidelines relevant to patient/client needs
Food and Nutrition Knowledge (BE-1.2) Potential Indicators • Level of knowledge (e.g. none, limited, minimal, substantial, and extensive • Areas of knowledge: • Food/nutrient requirements • Physiological functions • Disease/condition • Nutrition recommendations • Food products • Consequences of food behavior • Food label understanding/knowledge • Self-management parameters
Food and Nutrition Knowledge (BE-1.2) Measurement methods or data sources • Pre and post-tests administered orally, on paper, or by computer • Scenario discussions • Patient/client restate key information • Review of food records • Practical demonstration/test Typically used to monitor and evaluate change in the following domains of nutrition intervention: • Nutrition education, nutrition counseling