Download
1 / 49
580 likes | 1.66k Views
Angiotensin Receptor Blockers and Renoprotection in Diabetes. Denise Hughes Laurienti November 6, 2001. Clinical Case.

E N D
Angiotensin Receptor Blockers and Renoprotection in Diabetes Denise Hughes Laurienti November 6, 2001
Clinical Case A 54 y/o BF with DM, HTN and elevated protein/creatinine ratio on spot urine. She was started on an ACE I about 3 mo. ago. She returns today c/o dry cough for 2 months. She works as a telemarketer and can’t talk on phone without coughing. You suspect the ACE I. You want to know if switching her to an ARB would be appropriate.
Diabetes and Kidney Disease • Diabetes is the leading cause of ESRD in the US, Europe, and Japan • 40% of people with type II diabetes develop diabetic nephropathy • The risk of developing diabetic nephropathy is 10-20 times higher in patients with microalbuminuria (20-200 μg/min) compared to those with normoalbuminuria (<20 μg/min) • Diabetes accounted for 40% of patients with ESRD in the US between 1994 and 1998
Diabetes and Kidney Disease • 1st Stage – hyperfiltration • 2nd Stage – microalbuminuria • 3rd Stage – overt diabetic nephropathy • 4th Stage – advanced clinical nephropathy • 5th Stage – End-Stage Renal Disease
Development of Nephropathy • Normal Kidney – GBM prevents filtration of macromolecules such as albumin by charge and size barriers • In Diabetes – increased number of large pores and decreased heparan sulfate (major component of negative charge) allowing albumin to leak into urine
Development of Nephropathy Jamison, Wilkinson. Nephrology, 1997.
Screening for Microalbuminuria • Normal albumin excretion < 20 mg/day • Microalbuminuria 30-300 mg/day • Proteinuria does not show up on dipstick until protein excretion 300-500 mg/day • 24-hour urine collection is gold standard for detection of microalbuminuria • Microalbumin can be detected on urine sample if specified to lab (early morning sample ideal) • Protein/creatinine ratio is more accurate
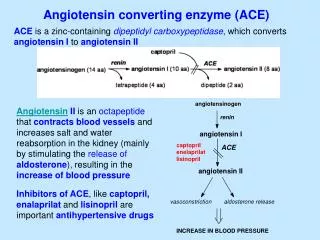
Renin-Angiotensin System AngiotensinogenAng I Ang II Ang Receptorrenin ACE binds to • Angiotensinogen produced and released by the liver • Renin produced by JG cells in response to glomerular hypoperfusion or changes in lytes • ACE produced mainly in pulmonary vasculature endothelium • Angiotensin II binds to its specific receptors in heart, brain, adrenal glands, kidneys, and vascular smooth muscle wall
Renin-Angiotensin System • Alternate pathways in which Ang I is converted to Ang II independent of ACE. Enzymes that facilitate this include chymase, CAGE, and cathepsin G. • Angiotensinogen can be directly converted to Ang II by t-PA, cathepsin G, or tonin. Zitnay, Siragy. Mineral Electrolyte Metabolism. 1998.
Renin-Angiotensin System There are 2 types of receptors to which Angiotensin II binds, and the effects differ: AT-1 receptors: • causes vasoconstriction • salt and water retention • aldosterone release and subsequent hypokalemia • sympathetic activity • stimulation of cell growth, proliferation, and matrix formation
Renin-Angiotensin System AT-2 receptors: • Less understood • Expressed mainly in fetal tissue • Thought to oppose actions mediated by AT-1 receptors • Lead to vasodilation, anti-proliferation, cell differentiation, apoptosis, and tissue regeneration
Pathways of AT-1 receptors thought to lead to protein phosphorylation Pathways of AT-2 receptors thought to lead to protein dephosphorylation Renal-Angiotensin System de Gasparo et al. Pharmacology Toxicology, 1998.
Mechanism of Action of ACE I and ARBs ACE I : • blocks conversion of Ang I to Ang II, so they diminish activity of AT-1 and AT-2 receptor subtypes • ACE is also a kininase so ACE I leads to increased kinin levels • Bradykinins cause vasodilation and lead to improved insulin sensitivity • Increased bradykinins cause common side effect of cough
Mechanism of Action of ACE I and ARBs ARBs: • Exhibit high affinity for AT-1 receptors and no effect on AT-2 receptors • AT-1 responsible for all of the deleterious actions of Ang II, so blocking it prevents vasoconstriction, salt and water retention, aldosterone release, and sympathetic activity • By blocking AT-1, some believe this will stimulate unopposed AT-2 leading to vasodilation
Evidence for ARBs and Renoprotection in Diabetes Three large RCTs looking at ARBs in patients with diabetes and their effectiveness at preventing nephropathy: • Renoprotective Effects of Irbesartan- irbesartan (2 different doses) vs. placebo • Irbesartan Diabetic Nephropathy Trial (IDNT)- irbesartan vs. amlodipine vs. placebo • Angiotensin II Antagonist Losartan Study (RENAAL)- losartan vs. placebo
Renoprotective Effect of Irbesartan Design: • randomized, double-blind, placebo controlled • 96 centers worldwide • Followed pts for 2 yrs • Parving HH, et al. The Effect of Irbesartan on the Development of Diabetic Nephropathy in Patients with Type II Diabetes. NEJM. 2001.
Renoprotective Effect of Irbesartan Patient Population: • Men and women age 30-70 • Type II diabetes • Hypertension- 2 of 3 blood pressure readings of SBP>135 and/or DBP>85 in one week • Persistent microalbuminuria- AER between 2 and 200 μg/min in 2 of 3 overnight urine specimens • SCr<1.6 mg/dl in men, <1.2 mg/dl in women • Exclusion of patients with nondiabetic renal disease, cancer, life expectancy<2yrs, or indication for ACE I
1469 Patients 3 wk screening process -128 patients -643 patients excluded for medical reasons albuminuria/BP out of range -18 patients no albuminuria 590 patients left for randomization Placebo Irbesartan 150 mg QD Irbesartan 300 mg QD N=201 N=195 N=194 Renoprotective Effect of Irbesartan
Renoprotective Effect of Irbesartan • Primary Endpoint: progression to overt nephropathy (AER>200 μg/min and 30% higher than baseline on 2 consecutive visits) • Secondary Endpoint: change in level of albuminuria, change in creatinine clearance, or normalization of albuminuria (to <20 μg/min)
Renoprotective Effect of Irbesartan Kaplan-Meier Curve showing the Incidence of Progression to Diabetic Nephropathy Parving HH, et al. NEJM. Sept., 2001
Renoprotective Effect of Irbesartan Conclusions: • Irbesartan 300 mg QD reduced risk of progressing to overt nephropathy and greater reduction in AER • Irbesartan 300 mg QD led to normalization of albuminuria in more patients • No significant difference in decline in creatinine clearance between the 3 groups
Irbesartan Diabetic Nephropathy Trial (IDNT) Design: • Randomized, double-blind, placebo controlled • 210 clinical centers • Mean duration of F/U 2.6 years • 1715 patients • Lewis EJ, et al. Renoprotective Effect of the Angiotensin-Receptor Antagonist Irbesartan in Patients with Nephropathy due to Type II Diabetes. NEJM. 2001
IDNT Patient Population: • Type II diabetic men and women age 30-70 • Hypertension SBP>135 and/or DBP>85 • Proteinuria >900 mg/24 hrs • Serum creatinine 1.0-3.0 mg/dl (women) and 1.2-3.0 mg/dl (men)
Primary Endpoint: Doubling SCr ESRD Death (any cause) Secondary Endpoint: Death (CV causes) MI CHF hospitalization CVA Above ankle amputation IDNT
IDNT - Results Patients in Irbesartan group had: • 23% lower rate of CHF than placebo • Increase in SCr 23% slower than placebo and 21% slower than amlodipine • 33% reduction of proteinuria compared to 6% in amlodipine group and 10% in placebo
IDNT - Results Adverse Events: Overall, irbesartan group had lower rate of adverse events/1000 days (P=0.002)
IDNT -Conclusions • Irbesartan assoc. with slowing of progression to nephropathy (decreased time to doubling of creatinine) • Results independent of blood pressure • Irbesartan assoc. with 23% lower rate of CHF • Lower adverse events in irbesartan group (but higher rate of hyperkalemia)
IDNT - Limitations • Bristol Myer Squibb performed data handling • Amlodipine used as comparison instead of diltiazem or verapamil • Patients in placebo group required more non-study antihypertensives, so more likely to receive B-blockers (United Kingdom Prospective Diabetic Study)
Angiotensin II Antagonist Losartan Study (RENAAL) Design: • Randomized, double-blind, placebo controlled • 250 centers in 28 countries • Followed 1513 patients for a mean of 3.4 years • Brenner BM, et al. Effects of Losartan on Renal and Cardiovascular Outcomes in Patients with Type II Diabetes and Nephropathy. NEJM. 2001
RENALL Patient Population: • Men and women age 31-70 • Type II diabetes • Nephropathy (alb/Cr ratio > 300 or AER>0.5 g/day on 24° urine) • SCr 1.3-3.0 mg/dl • Excluded-type I DM, nondiabetic renal dz, MI or CABG in last month, CVA or PTCA w/in 6 months, TIA in last year, or CHF
Primary Endpoint: Doubling of SCr ESRD Death Secondary Endpoint: MI Stroke Hospitalization for CHF or USA Vascular intervention Death from CV cause RENALL
RENALL – Results Patients in the losartan group had a reduction in proteinuria of 35%, while the patients in the placebo group had an increase in proteinuria (P=<0.001) Brenner et al. NEJM. 2001.
RENALL – Conclusions • Losartan has renoprotective effects by reducing risk of doubling creatinine AND by reducing progression to ESRD • Losartan reduces episodes of CHF • Effects reported as independent of blood pressure
ACE I versus ARBs Design: • Randomized, double-blind, placebo controlled • 4 centers in Canada • 122 patients followed for 52 weeks • Muirhead N, et al. The Effects of Valsartan and Captopril on Reducing Microalbuminuria in Patients with Type II Diabetes: A Placebo Controlled Trial. Current Therapeutic Research. 1999.
ACE I versus ARBs Patient Population: • Males and females > age 17 • Average age 50’s in all groups • Type II Diabetes • AER 20-300 μg/min, GFR > 60 ml/min • SBP<160 mmHg • Excluded-brittle DM, hypotension, DBP>95
ACE I versus ARBs Results: Primary Endpoint- Overt Nephropathy Secondary Endpoint- Change in GFR Most common adverse experience- cough (captopril)
ACE I versus ARBs Conclusions: • Patients in valsartan and captopril groups less likely to reach endpoint • No statistically significant difference between the valsartan and captopril groups
ACE I versus ARBs Limitations: • Small study population size • Differences among the groups • Lower AER initially in the captopril group • Short follow-up period
Final Conclusions Need for more evidence: • Unfortunate that these studies didn’t have ACE I as a treatment arm • HOPE and MICRO-HOPE show that ACE inhibitors reduce risk of CV events in patients with diabetes and one other risk factor for CV disease
Final Conclusions ARBs in heart failure: • ELITE II and Val-HeFT • Ongoing trials Dickstein. Current Controlled Trials in Cardiovascular Medicine. 2001.
Final Conclusions • ARBs are renoprotective in patients with diabetes • ARBs reduce risk of progression to overt nephropathy, rise in creatinine and ESRD • More evidence comparing ARBs and ACE I, and ARBs in diabetic patients at risk for CV disease is needed • ACE inhibitors still first line
Acknowledgments Special Thanks to: Dr. Pirouz Daeihagh Dr. Paul J. Laurienti







![>gi|14043064|ref|NP_114038.1| angiotensin II receptor, type 1 [Homo sapiens]](https://cdn2.slideserve.com/3772307/slide1-dt.jpg)