Download
1 / 31
370 likes | 993 Views
Hemodynamic Disorders (Disorders of blood flow). Dr. Abdelaty Shawky Dr. Gehan Mohamed. Infarction. * Definition: Development of an area of coagulative necrosis ( liquefactive in the brain) caused by acute cut of blood supply. * Causes: 1. Thrombosis. 2. Embolism.

E N D
Hemodynamic Disorders(Disorders of blood flow) Dr. Abdelaty Shawky Dr. Gehan Mohamed
* Definition: Development of an area of coagulative necrosis (liquefactive in the brain) caused by acute cut of blood supply. * Causes: 1. Thrombosis. 2. Embolism.
* Types of infarcts: 1. According to the color: a. Red infarcts (hemorrhagic): - Occur in vascular organs as the lung, liver and intestine. - The red color is due to hemorrhage in the substance of the infarct. b. Pale infarcts: - Are more common and occur in firm and less vascular organs as the kidney, heart and spleen.
2. According to the consistency: a. Firm: in all organs infarction except the brain. b. Soft: in brain and spinal cord infarction. 3. According to presence of absence of the bacteria: a. Septic infarction: in intestine. b. Aseptic infarction:
* Fate of the infarct: • Small infarct: Necrotic tissues are removed by macrophages, granulation tissue fills the defect followed by fibrosis. • Large infarct: Gets surrounded by a fibrous capsule and its substancemay show dystrophic calcification.
* Definition: Escape of blood outside the blood vessels or cardiac chambers.
* Causes of haemorrhage: 1. Trauma: involving the heart and blood vessels. 2. Diseases of blood vessels: a) Hypertension. b) Varicose veins: as piles. c) Degeneration: as atheroma and aneurysm. d) Infection: as tuberculosis. e) Malignant cells invading blood vessels. 3. Hemorrhagic blood diseases: as haemophilia, leukemia and scurvy.
* Types of haemorrhage: 1. External haemorrhage. 2. Internal haemorrhage 3. Interstitial haemorrhage
1. External haemorrhage Escape of blood outside the body. 1. Epistaxis:Bleeding from the nose. 2. Hemoptysis:Coughing of blood. 3. Hematemesis:Vomiting of blood. 4. Melena:Presence of dark digested blood in stools. 5. Bleeding per rectum:passage of red blood with stool
6. Hematuria:Blood in urine. 7. Menorrhagia:Excessive or prolonged menstrual bleeding. 8. Metrorrhagia:Irregular uterine bleeding unrelated to menses 9. Bleeding from skin
2. Internal haemorrhage Bleeding into body cavities. 1. Hemothorax:Hge into the pleural sac. 2. Hemopericardium:Hge. into pericardial sac. 3. Hemoperitoneum:Hge. into peritoneal sac. 4. Hematocele:Hge. into tunica vaginalis sac. 5. Hemoarthrosis:Hge. into a joint cavity.
3. Interstitial haemorrhage Bleeding into interstitial tissue spaces. 1. Petechial haemorrhage: escape of small amount of blood of capillary origin → small spots of haemorrhage. 2. Ecchymosis: escape of moderate amount of blood → a bigger patch of haemorrhage. 3. Hematoma: escape of large amount of blood causing a swelling.
- Interstitial haemorrhage is at first dark red (arterial blood) or bluish (venous blood). - Then, hemoglobin breaks down into biliverdin and hemosiderin. - BiIiverdin gives the area a green color but is soon absorbed in the blood. - The hemosiderin left gives the area a brown color and is gradually removed by macrophages, so the color changes to yellow and gradually fades away.
* Effects of haemorrhage: ● Small amount:No effect. ● Repeated small amounts (chronic hge): - Causes microcytic hypochromic anemia. - e.g. in piles and peptic ulcers. ● Massive amount: hemorrhagic shock.
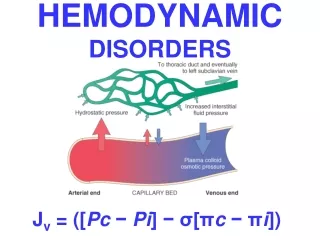
* Definition: - Pathological accumulation of excess fluids in the interstitial tissue spaces and serous sacs. - Edema fluid may be either transudate, exudate or lymph.
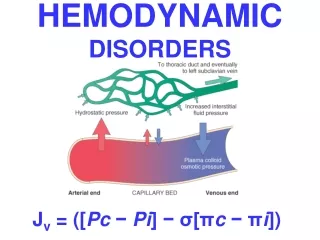
* Causes of edema: 1. Increased capillary hydrostatic pressure: occurs in cases of : - venous congestion (generalized or localized) - sodium & water retention → ↑ blood volume 2. Decreased plasma colloid osmotic pressure: occurs in cases of hypoproteinemia (fall of total plasma proteins below 2.5 gm% or fall of serum albumin below 1.5 gm%) 3. Increased capillary permeability: - Caused by toxins, hypoxia, & chemicals (e.g. histamine in acute infl.). - Escape of proteins into Interstitial fluid → ↓ plasma osmotic pressure & ↑ tissue osmotic pressure → further edema.
4. Lymphatic obstruction: - Lymphatic obstruction causes lymphatic edema (lymphedema). - It is caused by: 1- Lymphangitis and lymphadenitis as in Filariasis → elephantiasis. 3- Mechanical compression of lymphatics e.g. by tumors. 4- Lymphatic permeation by malignant cells. 5- Post-irradiation fibrosis in lymphatics & LNs. 6- Surgical removal of the lymph nodes.
* Classification of edema: 1. According to the site of edema: 1. Localized edema: e.g inflammatory edema, obstructive venous & lymphatic edema. 2. Generalized edema (anasarca): • Cardiac edema: due to heart failure • Renal edema: due to renal failure. • Nutritional edema: due to hypoproteinemia.
2. According to consistency of edema: 1. Pitting edema (Soft edema): in generalized edema and obstructive venous edema. 2. Non-Pitting edema (Hard edema): e.g in inflammatory edema and lymphatic edema.
Pitting edema • The accumulated fluid can be easily moved on pressing the affected part, leaving a pit at site of pressure (it pits on pressure). • This is because the edema fluid has low protein content → it is present free in the tissue spaces.
Non-Pitting edema • The edematous part does not pit on pressure. • This is because the edema fluid is united with the tissue elements. • Occurs in cases of lymphatic edema and inflammatory edema.
References: Robbins and Cotran’s: Pathologic Basis of Disease. Seventh edition.