Download
1 / 50
560 likes | 695 Views
Learn about Thyroid gland diseases including Hypothyroidism, Hyperthyroidism, clinical symptoms, causes, diagnosis, and treatment options. Understand the impact of Thyroid hormone deficiency during pregnancy and in the elderly.

E N D
Thyroid gland diseases Dr.Isazadehfar
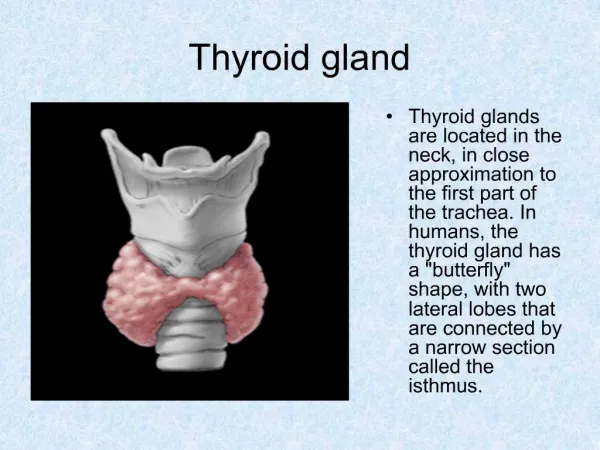
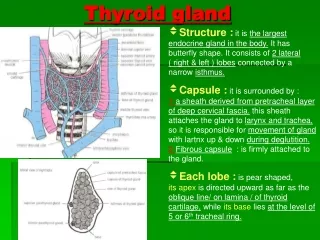
Synthesis and Secretion • Follicular cells arranged in clumps • Clumps of cells contain colloid • Colloid an iodine containing protein called thryoglobulin. This is the precursor and storage form of thyroid hormone • Thyroxine (T4), Triiodothyronone (T3)
Thyroid hormone action • T4 and T3 circulate in the blood bound to plasma proteins. • TBG(70%), TBPA(20%) and albumin(10%). • T3 is the active form, 5 times more active than T4. • T4 is converted to T3 outside the thyroid, mostly in liver and kidney. • T3 binds to a nuclear receptor
Regulation of the H-P-T axis • TRH secreted from hypothalamus controls TSH production. • TSH from anterior pituitary stimulates secretion of T4 and T3 from thyroid • Regulated by a negative feedback loop
Prevalence of Hypothyroidism • Prevalence is 14/1000 females and 1/1000 males • Other autoimmune diseases • Family history of autoimmune diseases
Primary hypothyroidism-Causes • Autoimmune thyroiditis (Hashimoto’s)(most common in adults) • Radioactive iodine • Post thyroidectomy • Anti-thyroid drugs (CMZ PTU) • Lithium - Amioderone • Iodine deficiency • Subacute thyroiditis • Infiltrative disease • Agenesis
Secondary hypothyroidism-causes • Hypothalamic disease • Pituitary disease
Tiredness Weight gain Cold intolerance Goitre Constipation Hair loss Bradycardia Angina Cardiac Failure Pericardial effusion Hypothermia Clinical featuresGeneral and CVS
Aches and Pains Carpal Tunnel Deafness Hoarseness Ataxia Depression Psychosis Iron deficiency A Pernicious Anemia Clinical FeaturesNeurological and Haematological
Dry skin Erythema Vitiligo Infertility Menorrhagia Galactorrhoea Amenorrhea Clinical FeaturesSkin and Reproduction
Laboratory Diagnosis • T4/FT4 reduced • T3/FT3 reduced • TSH elevated • Thyroid Antibodies may indicate aetiology • If TSH is reduced or normal in the presence of a low T4, pituitary function necessary
Additional abnormal tests • Fasting cholesterol and triglycerides may be raised • AST and LDH may be raised • CK , Chol , Triglyceride • Normochromic or macrocytic anemia • ECG: Bradycardia with small QRS complexes
Treatment • Levothyroxine • If no residual thyroid function 1.5 μg/kg/day • Patients under age 60, without cardiac disease can be started on 50 – 100 μg/day. Dose adjusted according to TSH levels • In elderly especially those with CAD the starting dose should be much less 12.5 – 25 μg/day • Compliance and adequacy of dose checked by TSH measurements • Try to maintain TSH in normal range
Subclinical Hypothyroidism • Primary thyroidal failure (Hashimotos) is a gradual process • Non specific symptoms • Reduced thyroid activity has been compensated by an increase TSH output to maintain a euthyroid state • Normal T4/FT4 with elevated TSH • Thyroid antibodies usually positive
Treatment • Repeat tests after an interval • If TSH is continuing to rise in the presence of strongly positive antibodies, the risk of developing hypothyroidism in the future is high. Thus treatment with thyroxin at this early stage may be justified if symptomatic • Beware: Thyroxine may not cure all symptoms
Myxoedema Coma • Requires prompt treatment. Mortality of 50%. • Suspect in cases of hypothermia • T3 20μg bid IM • Steroids recommended • Glucose to correct hypoglycaemia • Rewarming • Assisted ventilation
Thyroid hormone deficiency in Pregnancy • Goitre is common in pregnant women • TBG increased, thus total T4 and T3 increased. FT4 and FT3 are normal and TSH remains unchanged. • Hypothyroidism treated with thyroxin during pregnancy. Dose requirements increase. A change in dose usually needed each trimester.
Post-partum thyroiditis • Incidence is about 9%. • Transitory or permanent • Early hyperthyroidism ,later hypothyroidism ,euthyroid later. • Increased microsomal antibodies. • Thyroxine
Elderly • Non specific symptoms • Osteoporosis • Anemia • Heart Failure • Treatment with thyroxine • Start with small doses and titrate slowly. (25μg).
Summary • Suspicion • Women • Previous thyroid disease or treatment • Other autoimmune diseases • Elderly- caution with treatment
HYPERTHYROIDISM Prevalence Women 2% Men 0.2% 15% of cases occur in patients older than 60 years of age
Mechanism of Clinical Symptoms 1. Catabolism 2. Enhancement of sensitivity to catecholamines
Hyperthyroidism Symptoms • Hyperactivity/ irritability/ dysphoria • Heat intolerance and sweating • Palpitations • Fatigue and weakness • Weight loss with increase of appetite • Diarrhoea • Polyuria • Oligomenorrhoea, loss of libido
Hyperthyroidism Signs • Tachycardia (AF) • Tremor • Goiter • Warm moist skin • Proximal muscle weakness • Lid retraction or lag • Gynecomastia
Most common causes Graves disease Toxic multinodular goiter Autonomously functioning nodule Rarer causes Thyroiditis or other causes of destruction Thyrotoxicosis factitia Iodine excess (Jod-Basedow phenomenon) Struma ovarii Secondary causes (TSH or ßHCG) Causes of Hyperthyroidism
Graves Disease • Autoimmune disorder • Abs directed against TSH receptor with intrinsic activity. Thyroid and fibroblasts • Responsible for 60-80% of Thyrotoxicosis • More common in women
Graves Disease Eye Signs N - No signs or symptoms O – Only signs (lid retraction or lag) no symptoms S – Soft tissue involvement (peri-orbital oedema) P – Proptosis (>22 mm)(Hertl’s test) E – Extra ocular muscle involvement (diplopia) C – Corneal involvement (keratitis) S – Sight loss (compression of the optic nerve)
Graves Disease Other Manifestations • Pretibial mixoedema • Thyroid acropachy • Onycholysis • Thyroid enlargement with a bruit frequently audible over the thyroid
Onycholysis : softening of nails and loosening of nail beds • Low total cholesterol • Low HDL • Low total cholesterol/HDL ratio
Diagnosis of Graves Disease • TSH , free T4 • Thyroid auto antibodies • Nuclear thyroid scintigraphy (I123, Te99)
Treatment of Graves Disease • Reduce thyroid hormone production or reduce the amount of thyroid tissue • Antithyroid drugs: propyl-thiouracil, carbimazole • Radioiodine • Subtotal thyroidectomy → relapse 4-6 W after antithyroid therapy(euthyroid), pregnancy, young people? • Smptomatic treatment • Propranolol
Neoplastic Thyroid Disease • Thyroid Nodules • Goiter • Multinodular • Diffuse • Endemic • Thyroid Cancer • Well differentiated and poorly differentiated
Thyroid Nodular Disease • Thyroid gland nodules are common in the general population • Mainly in women • Most thyroid nodules are benign • Less than 5% are malignant • Only 8% to 10% of patients with thyroid nodules have thyroid cancer
Multinodular Goiter (MNG) • MNG is an enlarged thyroid gland containing multiple nodules • The thyroid gland becomes more nodular with increasing age • In MNG, nodules typically vary in size • Most MNGs are asymptomatic • MNG may be toxic or nontoxic • Toxic MNG occurs when multiple sites of autonomous nodule hyperfunction develop, resulting in thyrotoxicosis • Toxic MNG is more common in the elderly
Endemic Goiter • No longer a problem in the developed world • Still a serious health concern in parts of the world with iodine deficiency including mountainous areas or areas with high rainfall/flooding Kaplan, E. et al. Thyroid Disease Manager “Surgery of the Thyroid Gland” Chapter 21, May 99
Thyroid Carcinoma • Incidence • Thyroid carcinoma occurs relatively infrequently compared to the common occurrence of benign thyroid disease • Thyroid carcinomas • Papillary (70%) • Follicular (15%) • Medullary thyroid (5%) • Anaplastic carcinoma (5%) • Primary thyroid lymphomas (5%) • Metastatic from other primary sites (rare)
Risk factors for Malignancy • Solitary thyroid nodules in patients >60 or <30 years of age • Irradiation of the neck or face during infancy or teenage years • Symptoms of pain or pressure (especially a change in voice) • Male sex • Large Nodules (>3 or 4 cm) • Growth of nodule
Evaluating Thyroid Nodules • TSH measurement • Ultrasound of the thyroid • Fine needle aspiration • Radioactive iodine imaging
Thyroid Ultrasonography • Excellent for characterizing size and other features of nodule • Useful in localizing nodule for FNA • Cannot distinguish between benign vs. malignant
Thyroid FNA • Now considered the most cost effective and sensitive/specific diagnostic test of thyroid nodules • The use of US has expanded the role of FNA in evaluating nodules and improved the validity of the results
Typical Presentation of Thyroid Cancer • Painless lump • Normal thyroid function tests • Found on routine examination or by the patient • Slow growth or no growth over several months
Types of Thyroid Cancer • Papillary :develops from thyroid follicle cells in 1 or both lobes; grows slowly but can spread • Follicular :common in countries with insufficient iodine consumption; lymph node metastases are uncommon • Medullary: develops from C-cells, can spread quickly; sporadic and familial types • Anaplastic: develops from existing papillary or follicular cancers; aggressive, usually fatal • Lymphoma: develops from lymphocytes; uncommon
Papillary Thyroid Cancer • Most common type • Makes up about 70% of all thyroid carcinomas • Females outnumber males 3:1 • Highest incidence in women in midlife
Papillary Thyroid CancerCharacteristics • Unencapsulated tumor nodule with ill-defined margins • Tumor typically firm and solid • May present as nodal enlargement • Commonly metastasizes to neck and mediastinal lymph nodes • 40% to 60% in adults and 90% in children • <5% of patients have distant metastases at time of diagnosis • Lung is most common site
Follicular Thyroid Cancer • Second most common type of thyroid cancer • Solid invasive tumors, usually solitary and encapsulated • Usually stays in the thyroid gland, but can spread to the bones, lungs, and central nervous system • Usually does not spread to the lymph nodes Follicular Thyroid Cancer .
Medullary Thyroid Cancer • Tumor arising from the calcitonin-secreting C-cells of the thyroid gland • Mortality rate of 10% to 20% at 10 years • 20% to 30% are part of 3 familial autosomal dominant syndromes (MEN-2A, MEN-2B, or familial non-MEN medullary thyroid cancer [median age=21 years]) Medullary (C-cell) Carcinoma
Treatment of Thyroid Cancer Summary • Papillary and follicular thyroid cancer • Generally excellent prognosis • Risk for recurrence for as long as 30 years • Initial management • Surgery and radioactive iodine • LT4 suppressive therapy • Follow-up • Physical examination • Radioactive iodine scans • Serum Tg • TSH and T4