Download

1 / 20
230 likes | 839 Views
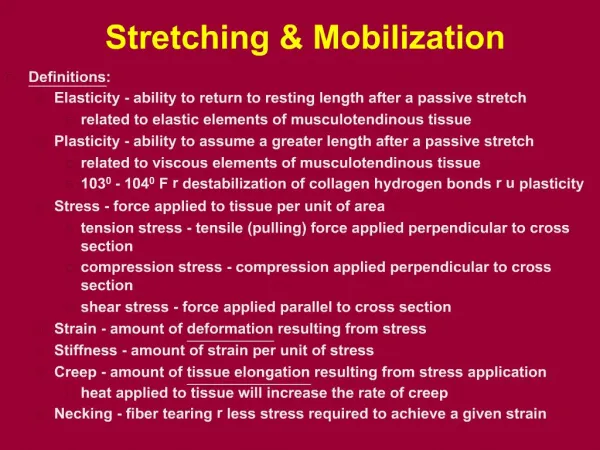
Neural mobilization Tests. Passive neck flexion (PNF). Straight leg raise (SLR). Prone knee bends (PKB). Upper limb tension tests (ULTT). Basic principles of tension testing.

E N D
Neural mobilization Tests • Passive neck flexion (PNF). • Straight leg raise (SLR). • Prone knee bends (PKB). • Upper limb tension tests (ULTT).
Basic principles of tension testing • A positive tension test does not constitute a definite indication to neural mobilization. Tension tests affect a lot of other structure as well as nerves. • Normal neural tissue which is being moved by testing may come into contact with sensitive interface structure and elicit pain.
Differential Diagnosis • To distinguish between origin of the symptoms the following should be considered: • Be aware of the expected normal response. • Know all details of all the symptoms. • Know the symptoms in the starting position.
Monitor symptoms throughout the procedures. Notice when pain starts. The effect of sensitizing additions/subtractions on the symptoms. This is considered an important factor to distinguish that the positive test is due to neural tissue affection.
Positive tension test • A tension test can be considered positive if • It reproduces the patient’s symptoms • The test response can be altered by movement of distant body parts • There are differences in the test from the left side to the right side.
Passive neck flexion (PNF) • Indications: • For all possible spinal disorders, headache symptoms, and for arm and leg pain of possible spinal origin. • Method: • The patient lies supine, arms are by the sides, and legs together. • The therapist takes the head into passive flexion on chest direction. • Normal response : • PNF is a painless test.
If patient felt pulling at the cervico-thoracic junction, this is related to muscle and joint rather than neuroaxis. Sensitizing addition For differentiation maintain PNF and adding SLR. If symptoms increase so it is neural if not so it is muscle or joint origin.
Sensitizing additions - Ankle dorsiflexion stress posterior tibial nerve. - Ankle planter flexion and inversion stress common peroneal nerve. - Hip adduction further sensitize sciatic nerve. - Hip medial rotation further sensitize sciatic nerve.
Prone knee bend • Indications: • Routine test for patients with knee, anterior thigh, hip and upper lumbar symptoms. Assessment of femoral nerve and its branches. • Method: • The patient lies prone, the therapist grasps the lower leg and flexes the knee to a predetermined symptoms response. • The response should be compared to the other side.
Normal response : Asymptomatic, and in some normal there is sensation of pulling or pain in the area of the quadriceps Sensitizing additions - Cervical flexion - Slump in side lying.
Upper limb tension test • Indications: • ULTT is recommended test for all patients with symptoms in the arm, head, neck and thoracic spine. Different test is provided to test each nerve (for example median nerve test, radial nerve test). • Method: • The patient is positioned in neutral supine • A constant depression of shoulder girdle is ensured during movement. • The shoulder is abducted to 110 degree. • With this position is maintained, • - The forearm is supinated and the wrist and fingers extended. • - The shoulder is laterally rotated. • - The elbow is extended.
Normal response : Deep stretch or ache in the cubital fossa, tingling sensation on the fingers Sensitizing additions With this position held, cervical lateral flexion to the left and then to the right is added
Treatment • After examination of the patient, if the therapist decides there is a relevant tension of the neural tissue, which need treatment. • One approach to that is the use of direct mobilization of the nervous system usually via tension tests and their derivatives.
Key to successful treatment • Nervous tissue mobilization fits perfectly into the Maitland concept. That is, the treatment of signs and symptoms based on the severity, irritability and nature of the disorder. • Treatment via neural mobilization is not a quickly acquired skill, nor is it an easy skill to learn.
Guidelines to the starting technique • Whatever the starting point used, the following should apply during the first technique application • The technique should be well away from the symptom area • Treatment should be non-provoking initially. • Maximal relaxation of the patient, and the painful areas will allow better nerve movement • If the technique starts to irritate the pain, either reduce the amplitude/range/speed of the technique. • After the initial mobilization, the symptoms must be reassessed.
Grading the technique • The grading of the technique is dependent on: • - Degree of irritability of the tissue • - The relationship between resistance to the movement and the symptoms received
Progression • The number of repetition of the technique may be as few as five or ten initially but can increase to many repetitions for several minutes. • Increasing the amplitude and taking the technique further into resistance. • Repeat the technique but alter to increase degree of tension by addition of the sensitizing components.
Contraindications • Recent onset of, or worsening neurological signs. • Cauda equine lesions • Cord signs. • Recent spinal surgeries