Download
1 / 35
370 likes | 481 Views
Inguinal Region. By Prof. Saeed Abuel Makarem. GROIN OR INGUINAL REGION. The groin or the inguinal region, extending between the ASIS and pubic tubercle. It is a very important area surgically and anatomically where structures enter and exit the abdominal cavity

E N D
Inguinal Region By Prof. Saeed Abuel Makarem
GROIN OR INGUINAL REGION • The groin or the inguinal region, extending between the ASIS and pubic tubercle. • It is a very important area surgically and anatomically where structures enter and exit the abdominal cavity • It is a potential site for herniation. • In fact, the majority of all abdominal hernias, occur in this region in particular the Inguinal hernia, which account for 80-90 % of all abdominal hernias.
Inguinal Canal • It is an oblique intramuscular slit in the lower medial part of the Anterior Abdominal Wall. • It runs just above and parallel to the medial part of the inguinal ligament. • Its length is about one & half inches (4 cm) in adult. • Its gives a passage for the spermatic cord in male, or round ligament of the uterus in female. • Also it gives a passage for the Ilioinguinal nerve in both sexes.
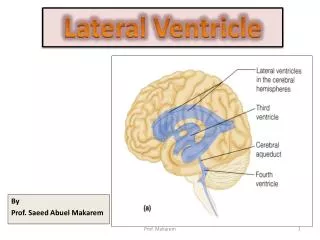
Inguinal Canal • Extends from the deep inguinal ring to the superficial inguinal ring • In the newborn child, the deep ring lies almost directly posterior to the superficial ring • The deep inguinal ring is an oval opening lies in the fascia transversalis • It lies ½ inch just above the midpoint of the inguinal ligament • Its margin gives attachment to the internal spermatic fascia.
Deep inguinal ring Superficial inguinal ring External oblique Medial Lateral
Boundaries of the Inguinal canal Ant. Wall: External oblique along whole length Internal oblique along lateral half. Post. Wall: Fascia Transversalis along whole length. Conjoint tendon (inguinal falx) along the medial part. Reflected ligament along medial ¼. Floor: Inguinal ligament supported medially by Lacunar ligament. Roof: Arching lower fibers of internal oblique.
The anterior wall is reinforced laterally by the origin of the internal oblique from the inguinal ligament • This wall is strongest where it lies opposite the weakest part of posterior wall, that is deep inguinal ring • The posterior wall is reinforced medially by the conjoint tendon. • This wall is strongest where it lies opposite the weakest part of the anterior wall, that is superficial inguinal ring
Spermatic Cord • Collection of structures that traverse the inguinal canal and pass to and from the testis • Covered by three layers of fascia derived from the layers of the abdominal wall • Begins at the deep inguinal ring, lateral to the inferior epigastric vessels, and ends at the testis
Contents of the Spermatic Cord • 1- Vas deferens: • Thick muscular tube transmitting sperms from the epididymis to the urethra • 2- Arteries: • A -Testicular artery (branch of abdominal aorta) • B-- Cremasteric artery (branch of inferior epigastric artery) • C-- Artery of the vas deferens (branch of inferior vesical artery) • 3- Veins: • Pampinioform plexus draining testis, continues as a single testicular vein, in the deep inguinal ring which drains into the inferior vena cava on right and into left renal vein on the left side
Contents of the Spermatic Cord • 4- Lymphatics: • Draining testis, pass through inguinal canal and drain into para-aortic lymph nodes. • 5- Nerves: • A. Autonomic nerves from renal and aortic plexuses, run with testicular artery • B - Genital branch of the genitofemoral nerve, which supplies the Cremasteric muscle • 6- Remains of the processus vaginalis
Coverings of the Spermatic Cord • Internal spermatic fascia, derived from the fascia transversalis • Cremasteric muscle and fascia: derived from the internal oblique muscle. • External spermatic fascia, derived from the external oblique aponeurosis
Scrotum • It is an out- pouch of the anterior abdominal wall • Formed of two pouches, fused in the midline • Contains testis, epididymis and lower part of the spermatic cord • Wall has following layers: • Skin • Dartos muscle • External spermatic fascia • Cremesteric fascia • Internal spermatic fascia • Tunica vaginalis
Scrotum • Skin is thin & wrinkled • Superficial fascia continuous with the fatty & membranous layers of the abdominal wall • In the fatty layer, fat is replaced by dartos muscle, a smooth muscle supplied by sympathetic nerves and responsible for wrinkling of skin of the scrotum
Scrotum Membranous layer is called Colle’s fascia It is continuous with the Scarpa’s fascia of the anterior abdominal wall • External spermatic fascia • Cremasteric muscle and fascia • Internal spermatic fascia • Tunica vaginalis: • Closed sac, derived from peritoneal cavity, covers the anterior, medial and lateral surfaces of testis
Testis • Mobile primary sex organ, lies in the scrotum • Left usually lies at a lower level than right • Each testis is surrounded by tough fibrous capsule, the tunica albuginea • Septae extending from capsule dividing the testis into lobules, which contain seminiferous tubules • Tubules open into rete testis, which are connected to epididymis through efferent ductules
Epididymis • 20 feet long, coiled tube, embeded in connective tissue forming a firm structure • Lies posterior to testis and lateral to vas deferens • Has head, body and tail. • Tail continues with the vas deferens • Is separated from the testis laterally by a groove lined by visceral layer of tunica vaginalis, called sinus of epididymis • It is called sinus of epididymis • Epididymis is the storage and maturation space for the spermatozoa
Lymphatic Drainage of Scrotum & Its contents • Skin, fasciae ,and tunica vaginalis: • drain into superficial inguinal lymph nodes • Testis and epididymis: drain into lumbar (para-aortic) lymph nodes.
Clinical Notes • Undescended testis • Anomalies of the processus vaginalis: • Hydrocele • Encysted Hydrocele • Hernias • Tapping of Hydrocele
Hernia • Hernia is the protrusion of part of abdominal viscera beyond the normal confines of the abdominal walls • It has three parts: • The sac • Contents of the sac • Coverings of the sac
Hernia: Types • Epigastric • Umbilical: congenital (Omphalocele) or acquired • Inguinal: • direct or indirect • Femoral • Incisional • Semilunar
Hernia: Types • Diaphragmatic or Hiatal • Lumbar Or (Petit’s triangle) • Obturator
Inguinal Hernia • Herniation of the abdominal viscera (usually small intestinal coils) through the inguinal region • It is of two type: • Direct • Indirect
Indirect Or oblique Inguinal hernia • Most common form of hernia • Most common in children & young adults • About 20 times more common in male than in female • 1/3rd are bilateral • More common on the right side
Indirect Inguinal hernia • Hernial sac: • Formed of remains of processus vaginalis • Enters inguinal canal through deep ring • Lies lateral to the inferior epigastric artery • Can be complete, extending to the scrotal sac, or incomplete, arrested in the inguinal canal
Direct Inguinal hernia • About 15% of inguinal hernia, • Rare in females • Common in old men with weak abdominal muscles • Hernial sac: • Bulges directly through the posterior wall of the inguinal canal i.e.through the inguinal (Hasselbach’s) triangle. This triangle is bounded medially by lateral edge of rectus abdominis muscle, laterally by inferior epigastric artery, infeiorly by inguinal ligament. • Lies medial to the inferior epigastric vessels • Usually nothing more than a generalized bulge
DIRECT INGUINAL HERNIA OBLIQUE INGUINAL HERNIA
Femoral Hernia • Protrusion of abdominal viscera through the femoral ring into the upper part of the thigh • More common in women (wider femoral ring) • Neck of the sac lies below and lateral to the pubic tubercle
Relation of inguinal & femoral hernial sacs to pubic tubercle • Inguinal: • sac lies above and medial to the pubic tubercle • Femoral: • sac lies below and lateral to the pubic tubercle
Management • Reduction of hernia (pushing the contents and the sac back to the abdominal cavity) • Repair of the weakness in the abdominal wall