Download
1 / 32
340 likes | 995 Views
CEREBRAL HEMISPHERE OR. CEREBRUM. By Prof. Saeed Abuel Makarem. CEREBRUM. It is the largest part of the forebrain. It is highly developed in human. It is derived from the telencephalon . The 2 cerebral hemisphere are incompletely separated by the median or greater longitudinal fissure.

E N D
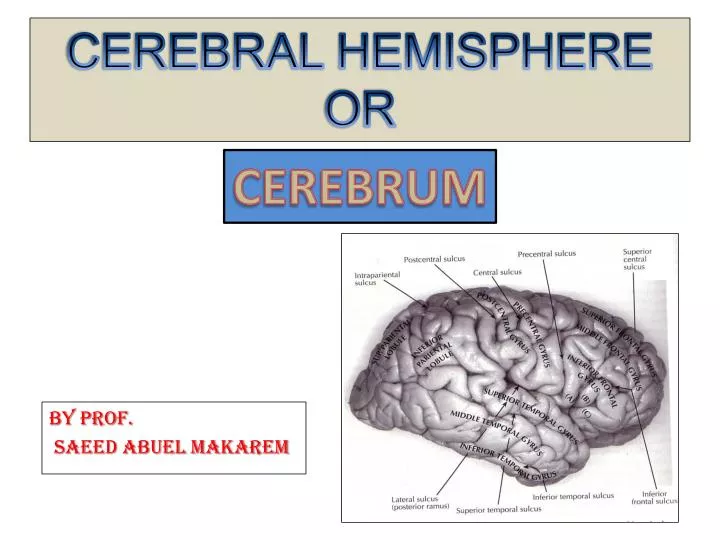
CEREBRAL HEMISPHEREOR CEREBRUM By Prof. Saeed Abuel Makarem
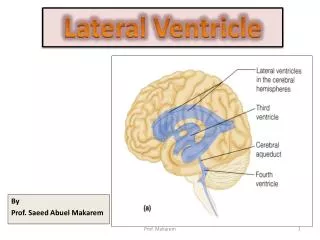
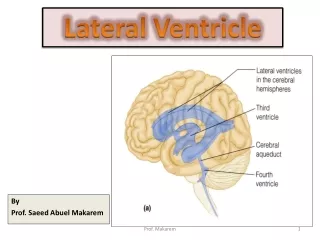
CEREBRUM • It is the largest part of the forebrain. • It is highly developed in human. • It is derived from the telencephalon. • The 2 cerebral hemisphere are incompletely separated by the median or greater longitudinal fissure. • They are connected by the corpus callosum. • Each hemisphere has a cavity called the lateral ventricle.
CEREBRUM : SURFACES • Each hemisphere has • 3 surfaces, • 3 poles, • 4 borders, • 4 Lobes. • Surfaces: • Lateral or superolateral: Convex and related to the skull vault. • Medial: • Flat & vertical and related to the falx cerebri & median longitudinal fissure. • Inferior: • Divided into orbital and tentorial parts by the stem of lateral sulcus.
CEREBRUM: BORDERS • Four borders: • 1- Medial or Superomedialborder: Between lateral & medial surfaces. • 2- Inferolateral border: Between lateral & inferior surfaces. • Its anterior part may be called superciliary border. • 3- Medial orbital border. • 4- Medial occipital border.
CEREBRUM3 POLES & 4 LOBES • Each hemisphere has 3 poles: • 1- Frontal pole. • 2- Occipital pole. • 3- Temporal pole. • Also, each hemisphere has 4 lobes: • 1- Frontal lobe. • 2- Temporal lobe • 3- Parietal lobe. • 4- Occipital lobe.
SULCI ON THE LATERAL SURFACE • Lateral sulcus or fissure: • Separates the frontal and parietal lobes from the temporal lobe. • Central sulcus: • Begins from the superomedial border ½ inch behind the midpoint between the frontal and occipital poles. • It descends downward & forward making an angle about 70▫ with the vertical line. • It stops slightly above the lateral sulcus. • Pre-central: a finger breadth anterior & parallel to the central sulcus. • Post-central: a finger breadth behind & parallel to the central sulcus. • Superior & inferior frontal sulci • Superior & inferior temporal sulci. • Interparietal sulcus. • Lunate sulcus
GYRI ON THE LATERAL SURFACE • Pre-central gyrus: Between central & precentral sulci. • Postcentral gyrus : • Between central & post-central sulci. • Superior, middle & inferior frontal gyri. • Superior, middle & inferior temporal gyri. • Superior & inferior parietal lobules. • Angular gyrus
SULCI ON THE MEDIAL SURFACE • Callosal sulcus: just above the corpus callosum. • Cingulate sulcus: one inch above & parallel to the callosal sulcus. • Parieto-occipital sulcus: begins in the upper border 4 cm in front of the occipital pole • It ends at the meeting of calcarine & postcalcarine sulci. • Calcarine: • Begins below the splenium then passes backwards and upwards to meet the parieto-ocipital sulcus then continuous as the postcalcarine sulcus. • Postcalcarine sulcus: It is an extension of the calcarine.
GYRI ON THE MEDIAL SURFACE • Cingulate gyrus: Between the callosal & cingulate sulci. • Paracentral lobule: • It is the continuation of the precentral & postcentral gyri. • Precuneus: behind the paracentral lobule. • Cuneus: between the parieto-ocipital & postcalcarine sulci. BODY G S
SULCI ON THE INFERIOR SURFACE • Olfactory sulcus: • Close & parallel to the medial orbital margin. • Orbital sulcus: • Irregular H- shaped lateral to olfactory sulcus. • Stem of lateral sulcus: • It divides the inferior Surface into, orbital & tentorial parts. • Rhinal sulcus: • A short sulcus on the temporal pole. • Collateral sulcus: • Behind the Rhinal sulcus and extends to the occipital pole. • Occipitotemporal sulcus: • Lateral to the collateral sulcus • It extends from temporal to occipital poles..
GYRI ON THE INFERIOR SURFACE • Gyrus rectus: • Medial to the olfactory sulcus. • Orbital gyri; • Anterior, posterior, medial and lateral, orbital gyri. • Lateral occipitotemporal gyrus: Lateral to occipitotemporal sulcus. • Medial occipitotemporal gyrus: Medial to occipitotemporal sulcus. • Parahippocampal gyrus: • Medial to collateral sulcus. • Lingual gyrus: • Between collateral & calcarine sulci. • Uncus: Anterior end of the Parahippocampal gyrus • It is the smell center.
IMPORTANT CENTERS OF THE CEREBRAL CORTEX OR MAIN FUNCTIONAL AREAS OF THE CEREBRAL CORTEX
The cerebral cortex is important for: Conscious awareness , Though, Memory and Intellect. Most sensory modalities ascend to the cortex from the thalamus, perceived & interpreted in the light of the previous experience.
Posterior part of the cerebrum receives sensory information in: 1- Parietal lobe (Somatosensory), 2- Occipital lobe (Vision), 3- Temporal lobe (Hearing). For identification by touch, sight & hearing. THEN ?
Storage & Retrieval of information • Information is elaborated to the association cortex, (at the meeting of the parietal, temporal & occipital) • The limbic system (medial part of cerebrum) enable storage & retrieval of the information processed in the posterior cortex.
MOTOR AREA • The frontal lobe (anterior part of cerebrum) is concerned with the • Organization of movement: • 1-Primary motor area. • 2-Premotor area. • 3-Supplementary motor area. • 4- Prefrontal area (guidance of complex motor behaviour).
PRIMARY MOTOR CORTEX (PMC) • In precentral gyrus & anterior part of the paracentral lobule. • It corresponds to Brodmann’s area 4 . • Body is represented upside down. • Size of the functional area is directly proportional to the skilled movement, not to the size of the muscle. • It is here that actions are conceived and initiated. • The principal subcortical afferent to PMC is from Lateral ventral nucleus (LVN) of thalamus. • LVN receives its input from globus pallidus & dentate nucleus.
Lesion:Upper 1/3 and paracentral lobule leads to affection of voluntary control in lower limb & perineum of the opposite side. • Lower 2/3rds: affection of voluntary control of the upper limb, & head, neck on the opposite side. • Isolated lesion of the premotor cortex leads to apraxia. • (Inability to perform skilled complex voluntary movement in spite of absence of muscle paralysis)
PREMOTOR CORTEX • Lies anterior to primary motor cortex. • Brodmann’s area 6. • It includes the posterior parts of superior, middle & inferior frontal gyri. • Function: • Programming & preparing for movement and control of posture. • It receives its afferent from ventral anterior nucleus of thalamus. 6
SUPPLEMENTARY MOTOR CORTEX • On the medial surface of the premotor cortex. • The principle subcortical input to premotor and supplementary motor cortex is the ventralanterior nucleus of the thalamus. • This nucleus receives its afferent from the globuspallidus & substantia nigra
FRONTAL EYE FIELD • It lies in posterior part of the middle fontal gyrus. • It is corresponding to; • Brodmann's area 8 • It controls conjugate movement of the eye. • Unilateral damage to area 8 causes conjugate deviation of the eyes to the side of the lesion.
MOTOR SPEECH AREABROCA’S AREA • In the inferior frontal gyrus in the dominant (usually left) hemisphere. • Brodmann’s areas 44 & 45 • It has connections with ipsilateral temporal, parietal, occipital lobes that share in language function. • Lesion: • (Left middle cerebral artery) • Expressive or motor aphasia (inability to express thought, answer or writing inspite of a normal comprehension)
PREFRONTAL CORTEX • The rest of the frontal lobe. • Lies anterior to premotor area. • It has rich connections with parietal, temporal and occipital cortex. • Functions: • Intellect. • Judgment. • Prediction. • Motivation • Planning of behaviour.
PRIMARY SOMATOSENSORY CORTEX • In the postcentral gyrus & posterior part of paracentral lobule. • It correspond to Brodmann’s areas 1, 2 and 3). • Here thalamocortical neurons terminate (3rd order neuron). • Input comes from ventral posterior nucleus (VPN) of the thalamus. • Within the somatosensory cortex the contralateral half of body is represented upside down.
VPN receives: • 1-Medial lemniscus • (Fine touch & proprioception). • 2-Spinal lemniscus • (coarse touch & pressure). • 3-Spiothalamic tract • (pain & temperature). • 4- Trigeminothalamic tract (general sensation from head)
PRIMARY AUDITORY CORTEX • Lies in the superior bank of the middle of the superior temporal gyrus. • Hidden within the lateral fissure. • Brodmann's 41, 42. • Its precise location is marked by small transverse temporal gyri ( Heschl’s convolutions). • Input to Primary auditory cortex is from medial geniculate nucleus (MGN) of the thalamus. • Auditory radiation undergoes partial decussation in the brain stem before it reaches the (MGN).
SECONDARY AUDITORY CORTEXorAUDITORY ASSOCIATION CORTEX • Lies behind the primary auditory cortex. • Continuous posteriorly with the second motor speech (Wernicke’s) area. • Here the heard sounds or words are interpreted. • Lesion: • Sensory aphasia; (inability to recognize the meaning of sounds or words with hearing unimpaired.
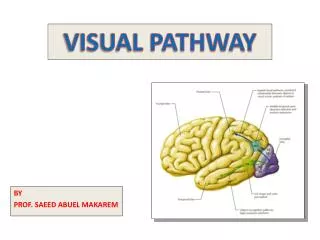
PRIMARY VISUAL CORTEX • Lies on medial surface of the occipital lobe. • In close relation to the calcarine sulcus. • It extends to the occipital pole. • Brodmann’s area 17 • It receives optic radiation from lateral geniculate nucleus (LGN) of the thalamus. • Each lateral half of the visual field is represented in the visual cortex of the contralateral hemisphere. • Lesion: Homonymous hemianopsia.
VISUAL ASSOCCIATION CORTEX • Brodmann’s areas 18,19 are called visual association cortex. • They are interpretive to the visual image. • Lesion: visual agnosia, (inability to recognize a seen object).
SECOND MOTOR SPEASCH AREA (Wernicke’s area) • Also, known as language area. • Lies in dominant hemisphere. • Lies in the inferior parietal lobule & auditory association area. • Lesion: • Sensory or receptive aphasia • (Lack of comprehension of words by vision or hearing)