Download
1 / 49
560 likes | 669 Views
Learn about the causes, risk factors, and clinical manifestations of kyphoscoliosis, a condition characterized by spinal curvature that affects lung function.

E N D
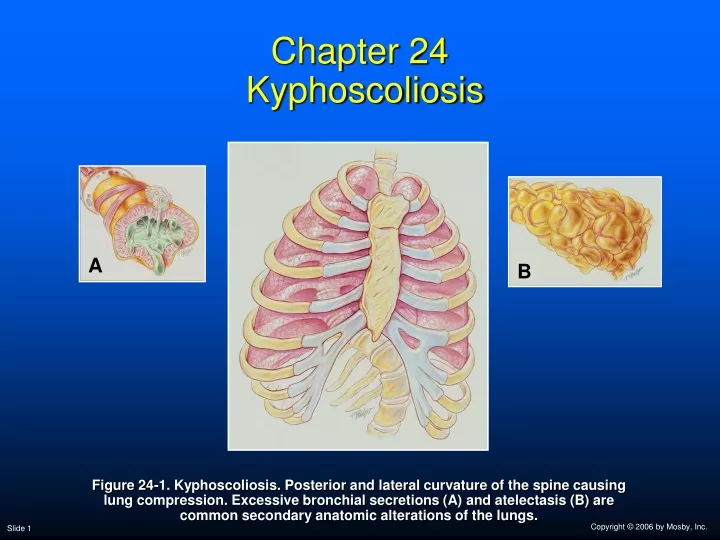
Chapter 24 Kyphoscoliosis A B Figure 24-1. Kyphoscoliosis. Posterior and lateral curvature of the spine causing lung compression. Excessive bronchial secretions (A) and atelectasis (B) are common secondary anatomic alterations of the lungs.
Anatomic Alterations of the Lungs • Lung restriction and compression as a result of the thoracic deformity • Mediastinal shift • Mucus accumulation throughout the tracheobronchial tree • Atelectasis
Etiology • Kyphoscoliosis affects about 2% of the people in the United States • Mostly young children going through growing spurts • Rarely develops in adults—unless a worsening condition from childhood • Kyphoscoliosis may also develop in adults from a degenerative joint condition in the spine
Etiology Associated with the following conditions: • Congenital connective tissue and skeletal disorders • Hormonal imbalance • Neuromuscular disorders • Trauma • Extraspinal contractures • Bone infections involving the vertebrae • Metabolic bone disorders • Joint disease • Tumors
Etiology Risk Factors • Sex—females are 10 times more likely than males to develop curvature of the spine • Age—the younger the child is when diagnosed, the greater the chance of curve progression • Angle of the curve—the greater the curvature of the spine, the greater the risk that the curve progression will worsen
Etiology Risk Factors • Location—in girls with lower back curvature, the curve is less likely to progress • Height—taller girls have a greater chance of curve progression • Spinal problems at birth—children with scoliosis at birth may experience a rapid curve progression
Etiology Clinically, scoliosis is commonly defined according to the following factors: • Shape • Nonstructural scoliosis—a side-to-side curve • Structural scoliosis—a curvature of the spine associated with vertebral rotation • Location • Thoracic • Lumbar • Thoracolumbar • Direction • Left or right curvature of the spine • Angle
Overview of the Cardiopulmonary Clinical Manifestations Associated with KYPHOSCOLIOSIS The following clinical manifestations result from the pathophysiologic mechanisms caused (or activated) by Atelectasis (see Figure 9-7) and Excessive Bronchial Secretions (see Figure 9-11)—the major anatomic alterations of the lungs associated with kyphoscoliosis (see Figure 24-1).
Figure 9-11. Excessive bronchial secretions clinical scenario.
Clinical Data Obtained at the Patient’s Bedside Vital signs • Increased respiratory rate • Increased heart rate, cardiac output, blood pressure
Clinical Data Obtained at the Patient’s Bedside • Cyanosis • Digital clubbing • Peripheral edema and venous distention • Distended neck veins • Pitting edema • Enlarged and tender liver • Cough and sputum production
Digital Clubbing Figure 2-46. Digital clubbing.
DistendedNeck Veins Figure 2-48. Distended neck veins (arrows).
Figure 2-47. Pitting edema. From Bloom A, Ireland J: Color atlas of diabetes, ed 2,London, 1992, Mosby-Wolfe.
Clinical Data Obtained at the Patient’s Bedside Chest assessment findings • Obvious thoracic deformity • Tracheal shift • Increased tactile and vocal fremitus • Dull percussion note • Bronchial breath sounds • Whispered pectoriloquy • Crackles, rhonchi, and wheezing
Figure 2-11. A short, dull, or flat percussion note is typically produced over areas of alveolar consolidation.
Figure 2-16. Auscultation of bronchial breath sounds over a consolidated lung unit.
Figure 2-19. Whispered voice sounds auscultated over a normal lungare usually faint and unintelligible.
Clinical Data Obtained from Laboratory Tests and Special Procedures
Pulmonary Function Study: Expiratory Maneuver Findings FVC FEVT FEF25%-75% FEF200-1200 N or N or N PEFRMVV FEF50% FEV1% N N or N N or
Pulmonary Function Study: Lung Volume and Capacity Findings VT RV FRC TLC N or VC IC ERV RV/TLC% N
Arterial Blood Gases Mild to Moderate Kyphoscoliosis • Acute alveolar hyperventilation with hypoxemia pH PaCO2 HCO3- PaO2 (Slightly)
Time and Progression of Disease Disease Onset Alveolar Hyperventilation 100 90 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors 80 70 60 PaO2 PaO2 or PaCO2 50 40 30 PaCO2 20 10 0 Figure 4-2. PaO2 and PaCO2 trends during acute alveolar hyperventilation.
Arterial Blood Gases Severe Kyphoscoliosis • Chronic ventilatory failure with hypoxemia pH PaCO2 HCO3- PaO2 Normal(Significantly)
Time and Progression of Disease Disease Onset Alveolar Hyperventilation Chronic Ventilatory Failure 100 Point at which disease becomes severe and patient begins to become fatigued 90 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors 80 70 PaCO2 Pa02 or PaC02 60 50 40 30 PaO2 20 10 0 Figure 4-7. PaO2 and PaCO2 trends during acute or chronic ventilatory failure.
Acute Ventilatory Changes on Chronic Ventilatory Failure • Acute alveolar hyperventilation on chronic ventilatory failure • Acute ventilatory failure on chronic ventilatory failure
Oxygenation Indices QS/QT DO2 VO2 C(a-v)O2 Normal Normal O2ER SvO2
Hemodynamic Indices (Severe Kyphoscoliosis) CVP RAP PAPCWP Normal CO SV SVICI Normal Normal Normal Normal RVSWI LVSWI PVRSVR Normal Normal
Laboratory findings • Complete blood count (CBC) • Elevated hemoglobin concentration and hematocrit if the patient is chronically hypoxemic
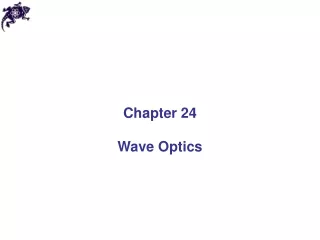
Radiologic Findings Chest radiograph • Thoracic deformity • Mediastinal shift • Increased lung opacity • Atelectasis in areas of compressed lungs • Enlarged heart (cor pulmonale)
Figure 24-2. Severe kyphoscoliosis in a 14-year-old male patient.
General Management of Kyphoscoliosis • Braces (25 – 45 degree curvature) • Milwaukee brace • Charleston brace • Boston brace • Wilmington brace • Thoracolumbosacralorthosis • Surgery (40 – 50 degree curvature) • Posterior spinal fusion and instrumentation • Anterior spinal fusion
General Management of Kyphoscoliosis Other approaches • Electrical stimulation • Chiropractic manipulation • Exercise to treat scoliosis
General Management of Kyphoscoliosis Respiratory care treatment protocols • Oxygen therapy protocol • Bronchopulmonary hygiene therapy protocol • Hyperinflation therapy protocol • Nocturnal mechanical ventilation
AnkylosingSpondylitis • Rheumatologic disease affects spine and thoracic cage • Dramatically decreases thoracic cage compliance
Review • A posterior curvature of the spine is called? • Kyphosis • A lateral curvature of the spine is called? • Scoliosis • Kyphoscoliosis affects approximately what percentage of the U.S. population? • 2% • What is the most common form of idopathickyphoscoliosis? • Adolescent Scoliosis
What is a nonstructural scoliosis? • A side-to-side curve that results from a cause other than the spine (poor posture, pain) • What is a structural scoliosis? • Curvature associated with vertebral rotation
True / False • Kyphoscoliosis is classified as an obstructive disorder. • False • Girl are 10 times more likely to develop curvature of the spine than boys. • True • Kyphoscoloiosis causes the patient’s PEFR to increase. • False
What was the patient’s P(A-a)O2? • Do we have enough information to calculate O2 content?
Effect of Acute Changes in PaCO2 on Bicarbonate • Increase in PaCO2 • Plasma HCO3- increases by 1 mEg/L for every 10 mm Hg PaCO2 > 40 mm Hg • Decrease in PaCO2 • Plasma HCO3- decreases by 2 mEg/L for every 10 mm Hg PaCO2 < 40 mm Hg