Download
1 / 41
820 likes | 4.09k Views
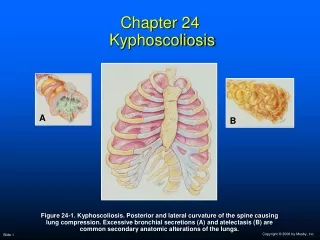
Chapter 24 Kyphoscoliosis. A. B. Figure 24-1. Kyphoscoliosis. Posterior and lateral curvature of the spine causing lung compression. Excessive bronchial secretions (A) and atelectasis (B) are common secondary anatomic alterations of the lungs. Anatomic Alterations of the Lungs.

E N D
A B Figure 24-1. Kyphoscoliosis. Posterior and lateral curvature of the spine causing lung compression. Excessive bronchial secretions (A) and atelectasis (B) are common secondary anatomic alterations of the lungs.
Anatomic Alterations of the Lungs • Kyphoscoliosis is a combination of two thoracic deformities that commonly appear together. • Kyphosis is a posterior curvature of the spine (humpback). • In scoliosis the spine is curved to one side—typically appearing as an S or C shape.
Anatomic Alterations of the Lungs (Cont’d) • Lung restriction and compression as a result of the thoracic deformity • Mediastinal shift • Mucous accumulation throughout the tracheobronchial tree • Atelectasis
Etiology • Kyphoscoliosis affects about 2% of the people in the United States • Mostly young children going through growing spurts • Rarely develops in adults—unless a worsening condition from childhood • Kyphoscoliosis may also develop in adults from a degenerative joint condition in the spine
Etiology (Cont’d) • Kyphoscoliosis is commonly associated with the following general conditions: • Congential scoliosis • Problem with the formation of the spine or fused ribs during fetal development • Neuromuscular scoliosis • Problems caused by poor muscle control, muscle weakness, or paralysis • Idiopathic scoliosis • Scoliosis from a unknown cause (80%-85% of the cases)
Etiology (Cont’d) • Idiopathic scoliosis is classified as follows: • Infantile scoliosis • The curvature of the spine develops during the first 3 years of life. • Juvenile scoliosis • The curvature occurs between 4 years and the onset of adolescence. • Adolescent scoliosis • The spine curvature develops after the age of 10.
Etiology (Cont’d) • Risk Factors Include: • Sex—Girls are more likely to develop curvature of the spine than boys. • Age—The younger the child is when the diagnosis is first made, the greater the chance of curve progression. • Angle of the curve—The greater the curvature of the spine, the greater the risk that the curve progression will worsen.
Etiology (Cont’d) • Risk Factors Include: • Location—Curves in the middle to lower spine are less likely to progress than those in the upper spine. • Height—Taller people have a greater chance of curve progression. • Spinal problems at birth—Children with scoliosis at birth (congenital scoliosis) have a greater risk of worsening of the curve.
Diagnosis • Scoliosis is diagnosed by means of the patient’s medical history, physical examination, x-ray evaluation, and curve measurement.
Diagnosis (Cont’d) • Clinically, scoliosis is commonly defined according to the following factors related to the curvature of the spine: • Shape • Location • Direction • Angle
Overview of the Cardiopulmonary Clinical Manifestations Associated with Kyphoscoliosis The following clinical manifestations result from the pathophysiologic mechanisms caused (or activated) by Atelectasis Excessive Airway Secretions
Clinical Data Obtained from Laboratory Tests and Special Procedures
PaO2 and PaCO2 trends during acute alveolar hyperventilation.
PaO2 and PaCO2 trends during acute or chronic ventilatory failure.
Figure 24-3. Severe kyphoscoliosis in a 14-year-old male patient.
General Management of Scoliosis The treatment of scoliosis largely depends on the cause of the scoliosis, the size and location of the curve, and how much more growing the patient is expected to do. In most cases of scoliosis (less than 20 degrees), the degree of abnormal spine curvature is relatively small and requires only observation to ensure that the curve does not worsen. Observation is usually recommended in patients with a spine curvature of less than 20 degrees.
In young children who are still growing, observation checkups are usually scheduled in 3- to 6-month intervals. When the curve is determined to be progressing to a more serious degree (above 25 to 30 degrees in a child who is still growing), the following treatments options are available: General Management of Scoliosis (Cont’d)
Braces Boston brace Charleston bending brace Milwaukee brace General Management of Scoliosis (Cont’d)
Figure 24-4 Common types of braces for scoliosis. A, Boston back brace (also called a thoraco-lumbro-sacral-orthosis [TLSO], a low-profile brace, or an underarm brace). Typically used for curves in the lumbar (low-back) or thoracolumbar sections of the spine. B, Charleston bending brace (also known as a part-time brace). C, Milwaukee brace (also called cervicothoracolumbosacral orthosis [CTLSO]) is used for high thoracic (mid-back) curves.
Surgery Spinal fusion Rod Instrumentation General Management of Scoliosis (Cont’d)
Figure 24-5 Radiograph of patient with scoliosis treated with a Harrington rod.
Other Approaches Some physicians may try electrical stimulation of muscles, chiropractic manipulation, and exercise to treat scoliosis. There is no evidence that any of these procedures will stop the progression of spine curvature. General Management of Scoliosis (Cont’d)
Other Approaches (Cont’d) Exercise, however, may improve the patient’s overall health and well-being. Prophylactic deep breathing and coughing (DB&C) exercises are also taught. Their long-term effect is debatable. General Management of Scoliosis (Cont’d)
Respiratory Care Treatment Protocols Oxygen Therapy Protocol Bronchopulmonary Hygiene Therapy Protocol Lung Expansion Therapy Protocol