Download
1 / 30
300 likes | 316 Views
This article discusses different types of cutaneous urinary diversions and examines extrophic anomalies in pediatric urology, including diagnosis, examination, treatment options, and goals of management.

E N D
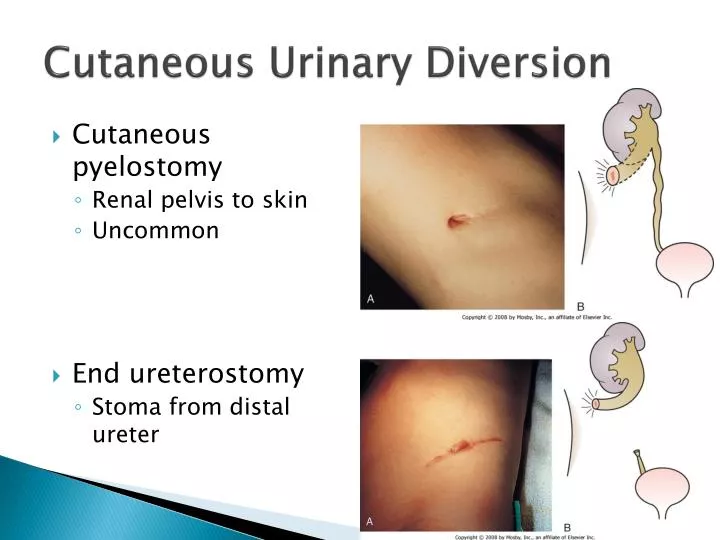
Cutaneous Urinary Diversion • Cutaneouspyelostomy • Renal pelvis to skin • Uncommon • End ureterostomy • Stoma from distal ureter
Cutaneous Urinary Diversion • Loop ureterostomy • Double barrel • Proximal and distal ureter • Intestinal diversion • Bowel between skin and ureters
Cutaneous Urinary Diversion • CutaneousVesicostomy • Most common • Bladder to skin • Appendicovesicostomy • Continent • Intermittent cath
Cutaneous Urinary Diversion • Nephrostomy • Catheter from upper urinary tract to skin
Question 4 You are called to the delivery room to evaluate a female baby with this defect which is located on the lower anterior abdominal wall. What is the most likely diagnosis? • Myelomeningocele • Cloacalextrophy • Hindgut extrophy • Prune belly syndrome • Classic bladder extrophy
Extrophic Anomalies • CloacalExtrophy • 1/200,000 • Rupture of cloacal membrane • Before urorectal septum completes descent to separate hindgut from bladder • Prognosis • Long-term survival 50%
Extrophic Anomalies • CloacalExtrophy • Exam • Bladder • 2 widely separate halves • Bowel mucosa in the middle • Ileocecal segment • Imperforate anus • Hypoplastic genitalia • Associated findings • Omphalocele • Myelomeningocele • Hydrocephalus
Extrophic Anomalies • Classic Extrophy • 1/40,000 • More common in boys • Premature rupture of the cloacal membrane • Exam • Red mucosal surface • Infraumbilical abdominal wall • Bladder as an open book • Inferior aspect ureteral orifices
Extrophic Anomalies • Classic Extrophy • Exam • Epispadias • Bifid or rudimentary penis • Normal or bifid scrotum • Inguinal hernias • Widespread pubic symphysis • Hemiclitoris • Duplicate vagina
Extrophic Anomalies • Classic Extrophy • Treatment • Keep bladder surface moist • Examine upper tract • Neonatal closure • Pelvic osteotomy
Extrophic Anomalies • Epispadias • 55% boys • Penopubic • Widened pubic symphysis • Broad spade-like penis • Urethra opened fully on dorsal surface to bladder neck • Dorsally tethered penis • Incontinent • Other boys • Penile or balaniticepispadias • Normal continence
Extrophic Anomalies • Epispadias • Girls • Rare • Incontinence • Wide urethra • Bifid clitoris • Treatment • Genitoplasty • Staged surgical correction • Renal U/S and VCUG
Urinary Retention • Acute • Usually voluntary • Associated with • Severe acute cystitis • Urethritis • Meatitis • Vaginitis • Other causes • Boys • Urethral stricture • Meatalstenosis with meatitis • Girls • Ureterocele
Urinary Retention • Other causes • Both • Bladder or urethral calculi • Masses - compression • Pelvic masses • Rhabdomyosarcoma • Uterine or ovarian masses • Hydro or hydrometrocolpos • Sacrococcygeal tumors • Constipation • Involvement of nerve roots • Spinal cord injury, tumor or transverse myelitis
Neurovesical Dysfunction • Meningocele • Myelomeningocele • Intradurallipoma • Diastematomyelia • Sacral agenesis • Trauma • Transverse myelitis • Spinal cord tumor Congenital Acquired
Neurovesical Dysfunction • Goals of management • Preserve renal function • Prevent renal damage from infection • Provide social continence • Evaluation • Radiographic or urodynamics • Several times in first year • Yearly thereafter • Warning signs • Infection • Fever • Change in continence
Non-NeurogenicVesical Dysfunction • AKA Hinman-Allen syndrome • Dysfunctional voiding • Features • Day and night incontinence • Fecal soiling • UTI • Behavioral problems • Detrusor/sphincter discoordination • Consequences • Incontinence • Renal failure
Non-NeurogenicVesical Dysfunction • Dysfunctional voiding • Diagnosis of exclusion • Must rule out • Tethered spinal cord • Infravesical obstruction • Treatment • Bladder retraining • Timed regimen • Biofeedback • Intermittent cath • Reverse complications • Temporary diversion • Renal function • Behavioral or psychological therapy
Question 5 The parents of a newborn male with the pictured physical exam finding inquire about circumcision. What do you tell them? • With their consent, you will proceed with circumcision • You will call the urologist and have him do the circumcision • Since they are medicaid, you will not perform the circumcision since it is no longer covered • Circumcision should be delayed in case the skin is needed for reconstruction • The patient needs immediate repair
Anomalies of the Male Genitalia • Hypospadias • 1/250 males • Location of meatus • Glanular • Coronal • Subcoronal • Distal shaft • Midshaft • Proximal shaft • Penoscrotal • Scrotal • Perineal • ? Chordee
Anomalies of the Male Genitalia • Hypospadias • Further work up • Cryptorchidism also? • Karyotype • VCUG? • Only with severe lesions or UTI • Renal U/S? • Proximal lesions • Treatment • Delay circumcision • Repair at 6 months
Anomalies of the Male Genitalia • Chordee • Ventral penile curvature • Uncommon without hypospadias • 3 possibilities • Skin tethering • Abnormal development of urethra and ventral penile structures • Congenitally short urethra • Treatment • Depends on cause • Delay circumcision
Anomalies of the Male Genitalia • Penile Torsion • Congenital or acquired • Most commonly mild • Median raphe spirals around shaft • Counterclockwise • May be seen after circumcision or hypospadias repair
Anomalies of the Male Genitalia • Webbed penis • Cosmetic • Transposition of scrotal skin onto the ventral penile shaft at the penoscrotal junction
Anomalies of the Male Genitalia • Buried penis • Most common after circumcision • Result of thick suprapubic fat pad • Resolves with normal development • Severe cases may require surgery
Postcircumcision Concerns • MeatalStenosis • Dysuria, strangury, deflected stream • Need to observe stream • Examination insufficient • Meatotomy under local anesthesia is curative • Meatal Bridge • Results from meatalstenosis in which ventral aspect recanalizes
Postcircumcision Concerns • Preputial adhesions and skin bridges • Fibrinous adhesions • Incomplete retraction of prepuce in normal development • Post-Circumcision • Complications • Disfiguring • Recurrent inflammation and infection • Trapped smegma • Surgical correction is complicated
Question 6 • Which of the following is the most accurate definition of micropenis in an infant? • A Penile stretch length <2cm • B Penile stretch length <1cm • C Penile length <2cm (not-stretched) • D Penile length <0.5cm (not-stretched)
Microphallus (Micropenis) • Stretch length <2cm (2 S.D. below mean) • 2 Causes • Hypogonadotropichypogonadism • (Failure of hypothalamus to produce GnRH) • Primary testicular failure • Deficient testosterone production • Requires extensive workup • Include karyotype, ?MRI of brain? • 3 month trial of testosterone
Diphallus • Usually associated with severe deformities of lower urinary tract and genitalia • Complete evaluation of upper and lower tract