Download
1 / 74
780 likes | 1.13k Views
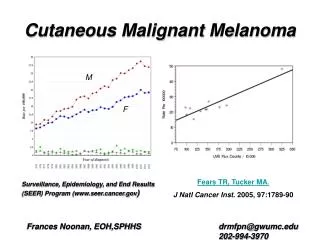
CUTANEOUS MELANOMA. MICHAEL STEFAN, M.D. SOUTHERN OHIO MEDICAL CENTER SCIOTO COUNTY MEDICAL SOCIETY 2/19/10. MOLE OR MELANOMA: EARLY DETECTION. LIFETIME RISK FOR THE DEVELOPMENT OF MELANOMA IS 1 IN 40 FOR 2010; UP FROM 1 IN 1500 IN THE 1935. ANNUAL NEW CASES ARE APPROXIMATELY 50,000.

E N D
CUTANEOUS MELANOMA MICHAEL STEFAN, M.D. SOUTHERN OHIO MEDICAL CENTER SCIOTO COUNTY MEDICAL SOCIETY 2/19/10
MOLE OR MELANOMA: EARLY DETECTION • LIFETIME RISK FOR THE DEVELOPMENT OF MELANOMA IS 1 IN 40 FOR 2010; UP FROM 1 IN 1500 IN THE 1935. ANNUAL NEW CASES ARE APPROXIMATELY 50,000. • IF SPREAD TO REGIONAL NODES ARE DISCOVERED, ONLY ONE THIRD WILL BE CURED. • ABCDE-A=ASYMMETRY; B=BORDER IRREGULARITY; C=COLOR VARIEGATION; D=DIAMETER >5MM AND E= ELEVATION. THE COMMON DENOMINATOR IS THEIR CHANGING NATURE WHICH SHOULD PROMPT EXCISIONAL BIOPSY. • HIGH VIGILANCE AND A LOW THRESHOLD FOR DERMATOLOGIC BIOPSY IS ESSENTIAL. • MOLES ARE A CLUSTER OF MELANOCYTES. MOST PEOPLE HAVE 10 – 40 MOLES.
A, B, C, D, E A SIMPLE TOOL FOR EVALUATION OF MOLES.
GROWTH PATTERNS OF MELANOMA • SUPERFICIAL SPREADING MELANOMA = 70% • NODULAR MELANOMA = 20% • LENTIGO MALIGNA MELANOMA = 10% IN ELDERLY POPULATION, MINIMAL PROPENSITY TO UNDERGO VERTICAL GROTH PHASE. • CONGENITAL NEVI • AMELANOTIC MELANOMA • UNKNOWN PRIMARY • 70% OF MELANOMAS FROM PRE-EXISTING NEVUS.
HISTOLOGIC GROWTH PATTERNS OF MELANOMA: • GROWTH PATTERNS; IMPORTANT BECAUSE THEY DETERMINE PROGNOSIS AND ARE DIVIDED INTO 4 PATTERNS: 1. SSM 2. NM 3.LMM 4. ACRAL LENTIGINOUS MELANOMA (ALM). 70% OF MELANOMAS ARE SSM AND MOST ARISE IN A PRE-EXISTING NEVUS. NM ACCOUNTS FOR 15-30% AND FREQUENTLY EVOLVE DE NOVO, MORE COMMON IN MEN AND AXIAL. LMMS CONSTITUTE 5% AND HAVE A LOW PROPENSITY FOR METASTASIS AND ARE ON THE FACE IN ELDERLY INDIVIDUALS. . UNCOMMON BEFORE AGE 50. ALMS OCCUR ON THE PALMS AND SOLES AND NAILBEDS. THEY ARE MORE COMMON IN PHENOTYPES 3 AND 4 ( MEDITERRANIAN, LATIN AND AFRO-AMERICAN).WHILE ALM ARE RARE THEY ARE AGGRESSIVE. • BIOLOGY OF MELANOMA – LOCATED AT THE EPIDERMAL-DERMAL JUNCTION, ARE OF NEURAL CREST ORIGIN AND ARE LOCATED ON THE SKIN IN 90%. ABOUT 4% OF MELANOMAS HAVE NO KNOWN PRIMARY SITE. THE TECHNIQUE OF MOLECULAR GENETICS HAVE BEEN USED TO IDENTIFY THE GENE ENCODING TYRONINASE SPECIFICALLY EXPRESSED IN MELANOCYTES. HMB-45 AND S-100 ARE HISTOLOGICAL MARKERS USED TO I.D. MELANOMA.
FAMILIAL AND SYNDROMIC MELANOMA • FAMILIAL MELANOMAS ARE UNCOMMON BUT HAVE BEEN WELL DOCUMENTED . THIS IS A AUTOSOMAL DOMINANT TRANSMISSION ORIGINALLY TERMED THE B-K MOLE SYNDROME AND NOW REFERRED TO AS THE DYSPLASTIC NEVUS SYNDROME., FAMILIAL TYPE. • MELANOMA SUSCEPTIBILITY GENES. 90% ARE SPORADIC; 7% FAMILIAL AND 3% HEREDITARY, THE HEREDITARY TYPE IS THE CDNK2A (P16) GENE CONTROLLING CELL GROWTH.
RISK FACTORS FOR MELANOMA : INTRINSIC MELANOCYTE : MELANOSOME : • SKIN • RETINA • MUCOSA • MENINGES • FOUND IN THE EPIDERMAL KERATINOCYTE • MSH-MELANIN STINULATING HORMONE DETERMINES PHENOTYPE OF PATIENT • FITZPATRICK PHENOTYPE IS CLASSIFIED FROM TYPE 1 THRU 5.
CUTANEOUSMELANOMA GENETICALLY SUSCEPTIBLE SUBPOPULATION PLUS CUMULATIVE LIFETIME ULTRAVIOLET RADIATION EQUALS MELANOMA RISK NOTE: GREATER THAN FIVE CHILDHOOD BURNS !
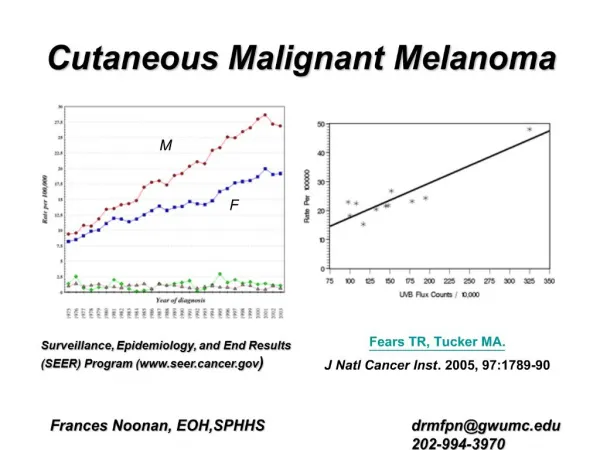
MELANOMA PROGRESSION • PUTATIVE STEPS IN PROGRESSION FROM A NORMAL MELANOCYTE TO MELANOMA: COMMON AQUIRED NEVUS…DYSPLASTIC NEVUS…INTRAEPITHELIAL PROLIFERATION OF ATYPICAL MELANOCYTES…MELANOMA IN SITU…SSM…VERTICAL GROWTH PHASE…METASTATIC • ONE OF THE BEST CHARECTERIZED GROWTH FACTORS FOR MELANOMA IS bFGF BASIC FIBROBLAST GROWTH FACTOR. SEVERAL MELANOMA CELL SURFACE MARKERS ARE PRESENT INCLUDING GANGLIOSIDE GD2 • AT LEAST 4 DISTINCT GENES LOCATED ON CHROMOSOMES 1,6,7 AND 9 MAY PLAY A ROLE IN MELANOMA.POSSIBLY A COMPLEX SET OF GENETIC EVENTS. CYTOGENIC ANALYSIS OF MELANOMA COULD BE USEFUL IN PREDICTING CLINICAL COURSE. • EXPOSURE TO SUNLIGHT IS CONSIDERED THE MAJOR CAUSE OF MELANOMA. THE IMMUNE SYSTEM MAY BE DEPRESSED BY UVB RAYS. HOWEVER, CUMULATIVE SUN EXPOSURE DOES NOT EXPLAIN ALL OF THE BIOLOGIC BEHAVIOR OF MELANOMA. THE HIGHEST INCIDENCE OF MELANOMA IS IN QUEENSLAND, AUSTRALIA
MELANOMA: CLINICAL WORK-UP • WORKUP: • CXR AND CT/PET SCAN- BLOOD CHEMISTRIES. • SERUM ALKALINE PHOSPHATASE AND LACTIC DEHYDROGENASE-PERHAPS OF HISTORICAL INTEREST ONLY. • BRAIN CT OR MRI • BONE SCAN • CONSULTATIONS BETWEEN ONCOLOGIST, RADIATION THERAPIST, GENERAL SURGEON AND PLASTIC SURGEON. • PROGNOSTIC FACTORS; BALCH 8500 PATIENTS UNIVARIANT AND MULTIVARIANT ANALYSIS FOR STAGE 1 AND 2 PRODUCING A RELATIONSHIP BETWEEN TUMOR THICKNESS AND 10 YEAR MORTALITY. • FOLLOW-UP EVERY 6 MONTHS. • RECURRENCE CAN OCCUR AS LATE AS 20 YEARS FOLLOWING PRIMARY DIAGNOSIS.
MELANOMA HISTORY • HISTORICALLY, THE FIRST PUBLISHED PATIENT WITH MELANOMA WAS BY JOHN HUNTER IN 1787. THE PATIENT WAS A 35 YEAR-OLD MALE. • RENE LAENNEC FIRST DESCRIBED MELANOMA AS A DISEASE ENTITY IN 1806. ( THEREFORE, NEARLY 200 YEARS OF UNDERSTANDING THE DISEASE.) • BIOLOGY, NATURAL HISTORY AND TREATMENT • THE CURRENT 5 YEAR SURVIVAL RATE OF 84% REPRESENTS A MARKED IMPROVEMENT OVER THE 60% RATE FOR THE YEAR 1960. • DYSPLASTIC NEVI ARE LARGER (>6MM ) THAN COMMON MELANOCYTIC NEVI AND THEIR PRESENCE SUGGESTS AN INCREASED INCIDENCE OF MELANOMA, EITHER IN THE DYSPLASTIC NEVUS OR IN UNINVOLVED SKIN.
MELANOMA MICROSTAGING • A MALIGNANT TUMOR OF MELANOCYTES, CELLS THAT ARE DERIVED FROM THE NEURAL CREST. • PREDOMINANTLY OCCUR IN ADULTS. • EARLY SIGNS IN A NEVUS INCLUDE DARKER OR VARIABLE DISCOLORATION, INTERVAL INCREASE IN SIZE, NODULARITY AND SYMPTOMATOLOGY; ITCHING, ULCERATION OR BLEEDING. • EXCISIONAL BIOPSY IS REQUIRED. THERE IS NO ROLE FOR INCISIONAL BIOPSY OR SHAVE BIOPSY AND AN EXPERIENCED DERMATOPATHOLOGIST IS REQUIRED FOR PROPER MICROSTAGING. • PROGNOSIS IS AFFECTED BY CLINICAL AND HISTOLOGIC FACTORS. • HISTOLOGIC FEATURES; THICKNESS OR LEVEL OF INVASION, MITOTIC INDEX, PRESENCE OF TUMOR INFILTRATING LYMPHOCYTES, SATELITOSIS
MICROSTAGING • DISTINGUISHING BETWEEN A BENIGN PIGMENTED LESION AND EARLY MELANOMA CAN BE DIFFICULT, AND EVEN EXPERIENCED DERMATOPATHOLOGISTS CAN HAVE DIFFERING OPINIONS. • THE MICROSTAGE OF MELANOMA IS DETERMINED BY 2 CLASSIFICATIONS ON HISTOLOGIC EXAMINATION. THE VERTICAL THICKNESS (BRESLOW) AS MEASURED BY A MICROMETER AND THE LEVEL OF INVASION WITHIN THE VARIOUS DERMAL LAYERS ( CLARK). • PATHOLOGIC STAGING INCLUDES MICROSTAGING OF THE PRIMARY MELANOMA AND PATHOLOGIC INFORMATION REGARDING THE REGIONAL LYMPH NODES AFTER SENTINAL NODE BIOPSY AND/OR LYMPHADENECTOMY. • DISCUSSION REGARDING MICROSTAGING
CLARK AND BRESLOW CLASSIFICATIONS: • CLARK CLASSIFICATION BASED ON DEPTH OF PENETRATION INTO PAPPILARY AND RETICULAR DERMIS. A MELANOMA BECOMES MALIGNANT WHEN IT PENETRATES THE BASEMENT MEMBRANE. THE SPREAD OF MELANOMA OCCURS IN THE SUPERFICIAL SUBCUTANEOUS TISSUE WHERE THE LYMPHATIC DRAINAGE IS LOCATED. • BRESLOW CLASSIFICATION- LESS SUBJECTIVE, MICROMETER IS USED TO MEASURE FROM THE GRANULAR LAYER TO THE DEEPEST POINT OF PENETRATION OF TUMOR CELLS. • BOTH CLASSIFICATIONS ARE REPORTED IN PATHOLOGY REPORT.
MULTIVARIATE ANALYSIS OF MELANOMA • MULTIFACTORIAL ANALYSIS-THICKNESS OF MELANOMA, ULCERATION, ANATOMIC LOCATION APPEAR TO BE THE MOST IMPORTANT. SEX, AGE AND TUMOR CHARACTERISTICS ALSO IMPORTANT. • HISTOLOGIC TUMOR CHARACTERISTICS OF LYMPHOCYTE INVASION, MICROSCOPIC SATELLITES, MITOTIC ACTIVITY AND LEVEL OF INVASION.
CUTANEOUSMELANOMA SURGICAL THERAPY
EXCISIONAL BIOPSY • FOLLOWING EXCISIONAL BIOPSY, THIN MELANOMAS ( < .76 mm ) ARE SURGICALLY TREATED WITH A 1.0 CM RADIAL EXCISION MARGIN. INTERMEDIATE DEPTH LESIONS ( .75 TO 2.0 mm ) ARE TREATED WITH A 2.0 RADIAL EXCISION. SOMEWHAT CONTROVERSIAL, PRIMARY LESIONS 2.0 TO 4 mm CAN BE TREATED WITH A 2.0 CM RADIAL EXCISION. MORE RADICAL TREATMENT OF THE PRIMARY SITE PROBABLY DOES NOT CONFER A SURVIVAL ADVANTAGE. LESIONS GREATER THAN 4 mm REQUIRE EXCISIONAL BIOPSY ONLY AND FURTHER THERAPY IS AIMED AT SYSTEMIC CONTROL BASED ON THE HIGH PREVELANCE OF ESTABLISHED SYTEMIC METASTASIS
SURGICAL TREATMENT • THE CORRECT SURGICAL TECHNIQUE FOR TREATMENT OF THE PRIMARY LESION INCLUDES A COMPOSITE RESECTION OF SKIN AND SUBCUTANEOUS FAT WITH PRESERVATION OF THE UNDERLYING FASCIA OR MUSCLE. REGARDLESS OF ANATOMIC LOCATION, FLAP RECONSTRUCTION OF THE POST-SURGICAL SITE IS PREFERRED. THERE IS NO ROLE FOR SKIN GRAFTING IN THIS REGARD. • PRIOR TO RESECTION OF THE PRIMARY LESION, ACCURATE IDENTIFICATION OF POTENTIALLY INVOLVED NODAL BASINS IS REQUIRED. LYMPHOSCINTIGRAPHY • MELANOMAS THAT HAVE A THICKNESS GREATER THAN 4.0 mm SHOULD BE CONSIDERED FOR ADJUVANT THERAPY WITH HIGH DOSE INTERFERON. TO DATE, THREE WELL DESIGNED PROSPECTIVE, RANDOMIZED CONTROLLED TRIALS DEMONSTRATED BOTH A DISEASE-FREE AND OVERALL SURVIVAL ADVANTAGE WITH INTERFERON WHEN COMPARED TO OBSERVATION OR ALTERNATE GANGLIOSIDE VACCINE. • ADJUNCTIVE CHEMOTHERAPY WITH MELPHALAN DOES NOT IMPROVE SURVIVAL . THE ONLY POTENTIAL DURABLE RESPONSE TO DISSEMINATED MELANOMA IS HIGH-DOSE INTERLEUKIN-2 (IL-2). • ALL PATIENTS WITH DISTANT METASTASIS ARE APPROPRIATELY CONSIDERED CANDIDATES FOR CLINICAL TRIALS EXPLORING NEW FORMS OF TREATMENT SUCH AS COMBINATION CHEMOTHERAPY, MONOCLONAL ANTIBODIES, IL-2, INTERFERONS, VACCINE IMMUNOTHERAPY AND BIOCHEMOTHERAPY.
WIDE LOCAL EXCISION OF AN INTERMEDIATE DEPTH MELANOMA:NOTE THE USE OF LYMPHAZURIN BLUE
SENTINAL LYMPH NODE MAPPING • SPONTANEOUS REGRESSION OF MELANOMA IS SEEN IN LESS THAN 1%. • INTERMEDIATE THICKNESS IS >.75 TO 2mm IN DEPTH. REGARDLESS OF THE BRESLOW DEPTH OF THE PRIMARY LESION IT IS SAFE TO SAY THAT ALL LESIONS CAN BE ADEQUATELY TREATED WITH A 2CM RADIAL MARGIN. ELECTIVE REGIONAL LYMPH NODE DISSECTION IS OF NO PROVEN BENEFIT IN STAGE 1 MELANOMA. HOWEVER, LYMPHATIC MAPPING AND SENTINAL LYMPH NODE BIOPSY FOR PATIENTS WHO HAVE TUMORS OF INTERMEDIATE THICKNESS MAY IDENTIFY THOSE PATIENTS WHO MAY BENEFIT FROM THERAPEUTIC LYMPHADENECTOMY. • ALTHOUGH PROPHYLACTIC REGIONAL LYMPH NODE DISSECTIONS HAVE BEEN USED IN PATIENTS WITH STAGE 11 MELANOMAS, 4 PROSPECTIVE RANDOMIZED TRIALS HAVE FAILED TO SHOW A SURVIVAL BENEFIT. IN FACT, TO DATE ELND AND TLND HAVE UNIVERSALLLY FAILED TO ABATE DISEASE PROGRESSION. FURTHERMORE, UNLIKE BREAST CANCER WHEREIN NODE DISSECTION IS OF VALUE FOR STAGING ONLY, RADICAL LYMPHADENECTOMY CARRIES A SIGNIFICANT OCCURRENCE OF PATIENT MORBIDITY.
LYMPHOSCINTIGRAPHY TECHNETIUM-LABELED SULFER COLLOID INJECTED AT THE PRIMARY CUTANEOUS MELANOMA SITE. THIS WILL IDENTIFY THE NODAL BASIN(S) THE MELANOMA IS DRAINING TO AND DIRECT THE SURGEON IN OBTAINING A SENTINAL NODE. FROZEN SECTION HISTOPATHOLOGY CANNOT BE PERFORMED ON THE PRIMARY LESION OR NODE. THE FALSE NEGATIVE RATE FOR SENTINAL NODE BIOPSY IS 3%.
SENTINAL LYMPH NODE BIOPSY • THE DIAGNOSTIC ACCURACY OF SENTINAL LYMPH NODE BIOPSY (SLNB) HAS BEEN DEMONSTRATED IN SEVERAL STUDIES., WITH A FALSE NEGATIVE RATE <2%. USING A VITAL BLUE DYE AND A RADIOPHARMACEUTICAL AGENT INJECTED AT THE SITE OF THE PRIMARY TUMOR. THE FIRST LYMPH NODE THAT DRAINS THE NODAL BASIN CAN BE IDENTIFIED AND EXAMINED FOR MICROMETASTASIS. IF MICROMETASTASIS IS FOUND BY THE DERMATOPATHOLOGIST, ELND CAN BE PERFORMED. HOWEVER, THERE IS NO PROVEN SCIENTIFIC EVIDENCE THAT ELND IN THE SETTING OF MICROMETASTASIS WILL IMPROVE DISEASE FREE SURVIVAL. THESE PATIENTS MAY BENEFIT FROM INTERFERON THERAPY AND IT IS PERHAPS HERE, THAT SLNB IS OF VALUE. • THE OVERALL MEDIAN SURVIVAL FOR PATIENTS TREATED WITH HIGH DOSE INTERFERON WHEN COMPARED WITH CONTROLS IS 3.8 YEARS.
SENTINAL LYMPHADENECTOMY IN CUTANEOUS THIN MELANOMAS :RICHARD BLEICHER, JOHN WAYNE CANCER INSTITUTE • HIGHLY ACCURATE AND MINIMALLY MORBID • FOLLOWING LYMPHOSCINTIGRAPHY, LYMPHATIC MAPPING AND SENTINAL LYMPADENECTOMY (LM/SL) WAS PERFORMED USING BLUE DYE ALONE OR WITH RADIOPHARMACEUTICAL • 512 PATIENTS INSTITUTIONAL REVIEW FROM 1985-2000. • THE RATE OF SN POSITIVE WAS 7.1% IN LESIONS BETWEEN 1.01 AND 1.5mm. FOR THE 272 PATIENTS WITH LESIONS < 1.00mm 2.9% WERE SN POSITIVE AND 1.7% OF PATIENTS WITH LESIONS < .75 mm HAD NODAL METS. PATIENTS WITH POSITIVE NODES TENDED TO BE YOUNGER
SENTINAL LYMPHADENECTOMY IN CUTANEOUS THIN MELANOMAS :RICHARD BLEICHER, JOHN WAYNE CANCER INSTITUTE • CONCLUSIONS; LM/SL IS INDICATED IN ALL PRIMARY LESIONS > 1mm AND YOUNG AGE MAY CORRELATE WITH NODAL METS IN LESIONS < 1.0 mm. FOR LESIONS <.75 LM/SL IS RARELY INDICATED, HOWEVER, SHOULD BE CONSIDERED IN NODULAR PRIMARY AND IN YOUNG AGE, (<40 YEARS OLD)
CUTANEOUS MELANOMA • CASE STUDIES
FACIAL MELANOMA SSM- “FIELD OF FIRE” DISSECTIONWITH MUSTARDE FLAP