Download
1 / 24
350 likes | 1.1k Views
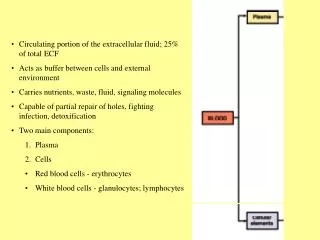
Regulation of Extracellular Fluid Osmolarity and Sodium Concentration. Excretion of excessive water by forming a dilute urine. The kidneys can excrete urine with an osmolarity as low as 50 mOsm/L (1/6 of normal urine osmolarity)

E N D
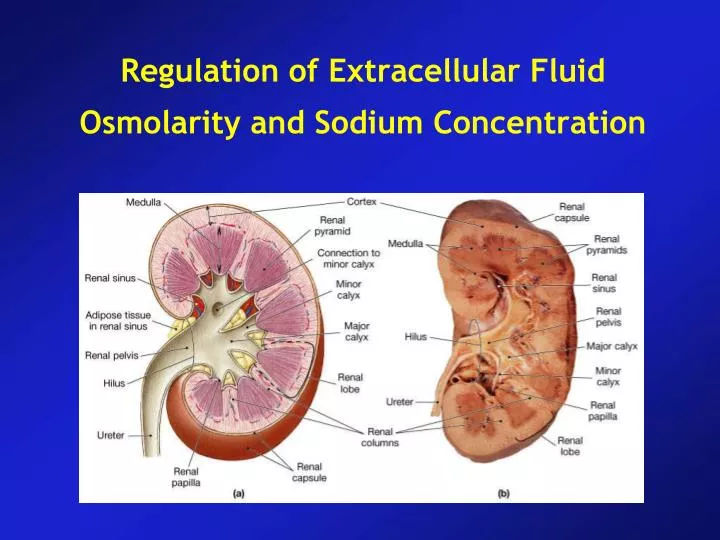
Regulation of Extracellular Fluid Osmolarity and Sodium Concentration
Excretion of excessive water by forming a dilute urine • The kidneys can excrete urine with an osmolarity as low as 50 mOsm/L (1/6 of normal urine osmolarity) • Conversely, when there is a deficit of water and extracellular fluid osmolarity is high, the kidney can excrete a urine with osmolarity as high as 1200-1400 mOsm/L • Role of anti-diuretic hormone (Vasopressin) in concentrating urine
Generating a dilute urine from: Guyton, AG & Hall, JE, Medical Physiology (10th Ed.), 2000, Chp. 28. • A dilute urine results from the reabsorption of salt from tubule segments • impermeable to H2O.
Excretion of Concentrated Urine • Ability of the kidney to form a more concentrated urine is essential for survival • It is achieved by increased water reabsorption and increased solute excretion • Obligatory urine volume • A normal adult must excrete about 600 mOsm of solutes per day • If the maximal urine concentration ability is 1200 mOsm/L, the minimal volume of urine that must be excreted: • 600 mOsm L/ 1200 mOsm L = 0.5 L/ Day
Requirements for excreting a concentrated urine • High ADH levels • Hyperosmotic renal medulla which provides the osmotic gradient necessary for water reabsorption to occur in the presence of high levels of ADH
Generating a concentrated urine • A concentrated urine results from the reabsorption of H2O (by osmosis) • from tubule segments that are exposed to a hyperosmotic interstitium.
Requirements for excreting a concentrated urine • Major factors that contribute to the buildup of solute concentration in the renal medulla: • Active transport of Na ions and co-transport of K, Cl and other ions out of the thick portion of Henle • Active transport of ions from the collecting ducts into the medullary interstitium • Facilitated diffusion of urea from the medullary collecting ducts into the medullary interstitium • Diffusion of only small amounts of water from the medullary tubules into the medullary interstitium
Countercurrent Mechanism Produces a Hyperosmotic Renal Medullary Interstitium
Countercurrent Mechanism Produces a Hyperosmotic Renal Medullary Interstitium • Countercurrent multiplication • Between ascending and descending limbs of loop • Creates osmotic gradient in medulla • Facilitates reabsorption of water and solutes before the DCT • Permits passive reabsorption of water from tubular fluid
Role of distal tubule and collecting ducts in excreting a concentrated urine
Urea Contributes to Hyperosmotic Renal Medullary Interstitum and to a Concentrated Urine
Preservation of Hyperosmolarity by Vasa Recta 1) Medullary blood flow is low 2) The vasa recta serves as countercurrent exchangers • The vasa recta does not create the hyperosmolarity, but they do prevent it from being washed away
The vasa recta • The vasa recta are hairpin- • shaped vessels that run • parallel to the loop of Henle.
Urine Concentration Mechanism http://www.cellphys.ubc.ca/undergrad_files/urine.swf http://www.youtube.com/watch?v=XbI8eY-BeXY http://www.youtube.com/watch?v=AOqIlrQhqHQ
Disorders of Urinary Concentrating Ability 1) Inappropriate secretion of ADH 2) Impairement of countercurrent mechanism 3) Inability of the distal tubule, collecting tubule and collecting ducts to respond to ADH • Failure to produce ADH (Central diabetes insipidus) • Inability of the kidneys to respond to ADH (Nephrogenic diabetes insipidus)
Control of Extracellular Fluid Osmolarity and Na Concentration • Osmoreceptor – ADH feedback system
ADH Synthesis in Supraoptic and Paraventricular Nuclei of the Hypothalamus and ADH release from the posterior pituitary
Cardiovascular reflex stimulation of ADH release by decreased Arterial Pressure and/or decreased blood volume • Decreased arterial pressure and / or blood volume • Arterial baroreceptor reflexes • Cardiopulmonary reflexes
Role of Thirst in Controlling Extracellular Fluid Osmolarity and Sodium Concentration • CNS centers for thirst – hypothalamus – anteroventral wall of the 3rd ventricle • Stimuli for thirst: increased extracellular fluid osmolarity • Salt-apetite mechanism for controlling extracellular fluid Na concentration and volume • There are two primary stimuli to increase salt apetite: • Decreased extracellular fluid Na concentration • Decreased blood volume or blood pressure associated with circulatory insufficiency
Control of Extracellular Fluid Sodium Concentration: ADH and Thirst