Download
1 / 54
710 likes | 1.45k Views
Infection of female reproductive system. Jun Ma Dept. of Obstetrics & Gynecology The First Hospital of Xi’an Jiaotong Univ. Overview. Anatomical feature of the female pelvic organs: Presence of a natural defense system Among the most important problems encountered in clinical practice

E N D
Infection of female reproductive system Jun Ma Dept. of Obstetrics & Gynecology The First Hospital of Xi’an Jiaotong Univ
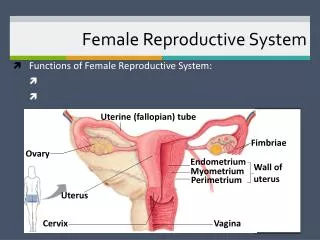
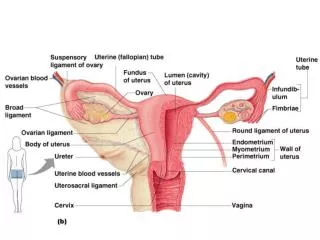
Overview • Anatomical feature of the female pelvic organs: • Presence of a natural defense system • Among the most important problems encountered in clinical practice • Infection of lower genital tract: irritating, indicative of STD, reflect the presence of genital tract malignancy • Inflammation of the upper genital tract: menstrual disorders, chronic pelvic pain and dyspareunia, and sterility
Affected organs: external genitalia: internal genitalia: • Localized or disseminated • Stage of infection: acute, subacute, recurrent, chronic
Etiology 1. Causative agents • Bacteria • Virus • Fungi • Parasite • Chlamydia • Protozoon • Spirocharta
Etiology 2. Disequilibrium of vaginal environment • Endogenous flora: lactobacilli, acidogenic corynebacteria, small quantities of candida • Estrogen------large quantities of glycogen------increased production of lactic acid-----PH 3.8-4.2--------promote the growth of normal vaginal flora • Frequent intercourse • Frequent vaginal douche • Disturbance of endogenous flora • Abuse antibiotis
Etiology 3.Absence or diminish of endogenous estrogen in adolescent and postmenopausal period 4. Allergy or irritation response 5. Diminished immunity 6. Urinary and fecal soiling
Evaluation • History: current symptoms, age, sexual activity, use of feminine hygiene products, medications, diabetes, overlying garments • Common manifestation: vaginal discharge and vulvar pruritus • Inspection • Tests: pH, 10% KOH or normal saline test, selective culture for pathogens
Nonspecific Vulvitis Etiology Any woman with certain allergies, sensitivities, infections, or diseases can develop vulvitis • Scented, colored toilet paper, perfumed soaps or bubble baths • Shampoos and hair conditioners • Laundry detergents (especially enzyme-activated "cold water" formulas) • Vaginal sprays, deodorants, douches, and powders • Spermicides
Nonspecific Vulvitis • Douches that are too strong or used too frequently • Hot tub and swimming pool water • Synthetic undergarments without a cotton crotch • Rubbing against a bicycle seat, horseback riding • Wearing a wet bathing suit for a long period of time • Glycosuria
Clinical manifestation • Redness and swelling on the labia and other parts of the vulva • Excruciating itching • Clear, fluid-filled blisters (present when the vulva is particularly irritated) • Sore, scaly, thickened, or whitish patches (more prevalent in chronic vulvitis) on the vulva
Diagnosis • Blood tests • Urinalysis • Tests for sexually transmitted diseases (STDs) • Pap test • Skin scraping or biopsy • Patch test
Treatment for vulvitis • Perineal hygiene, withdrawal of irritating substance • Occasional douching with warm water or acidic solution • Topical corticosteroids, oral antihistamines, Xylocaine 2% jelly • Estrogen vaginal cream • Eliminate cause
What is the anatomical location of Bartholin’s glands • Bartholinitis: inflammation of one or both gland or ducts • Causative agents: staphylococci, gonococci, E. coli, STD pathogens
Pathogenesis • Infection intrudes through the outward glandular duct (canaliculitis) ------ spreads to the parenchyma (serous, purulent inflammation)------false abscess Outcomes recurrent, persist, Bartholin’s cyst • Complete drainage • Incomplete drainage • Infection abate
Clinical manifestation • Malaise, weakness, swollen feeling in the external genitals, rising temperature ( acute phase ) • Swelling and hyperemia, tenderness, hectic temperature, chills (false abscess), • Retention cyst (chronic phase), tendency to recur
Treatment • Early stage: antibiotic, analgesics, hot bath • Abscess formed: complete drainage marsupialization---pouch making • Antibiotic + pus culture • “Bartholin’s cyst” in women of > 50 ys, biopsy is recommended.
Bacterial vaginosis • The most common cause of vaginitis during childbearing years (40-50%) • Multiple sexual partners increases the risk • STD? • Caused by disequilibrium of normal vaginal bacteria • High numbers of Gardnerella vaginalis, Mycoplasmahominis, Bacteroides species, and Mobiluncus species • Low numbers or disappearance of Lactobacillus
Consequence • Used to be considered inconsequential • Associated with PID, postabortion endometritis, posthysterectomy vaginal cuff infection, chorioamnionitis, postpartum endometritis, PROM, preterm labor
Symptoms, Signs • Malodorous discharge • Itching and irritation • Amine (fishy) odor , stronger after coitus and menses • Redness and edema are uncommon
Diagnosis "Amsel's criteria”:presence of three of four criteria • A thin, milky white discharge • Whiff test: presence of a fishy odor revealed by 10% potassium hydroxide wet mounts • Vaginal pH of > 4.5 • Presence of "clue cells”: bacteria adherent to epithelial cells • Presence of WBCs: gonorrhea or chlamydial infection, cultures should be performed
Treatment • Metronidazole: 250 mg tid or 500 mg bid for 7 days • Metronidazole vaginal gel 0.75% daily for 5 days • Clindamycin 2% vaginal cream daily for 7 days • Treatment for sexual partners not recommended by CDC
Candida vulvovaginitis • Vulvovaginal candidiasis, Candidal vaginitis, monilial infection, or vaginal yeast infection • 20-25% of vaginitis, 75% of all women have at least once infection • Overgrowth of Candida albicans or other sp. of Candida • Not included in STD • Predisposing factor: pregnancy, diabetes, OC, antibiotics, poor hygiene, immunosuppression • Recurrent vaginal candidiasis: > four attacks/year
Symptoms, Signs • Vaginal pruritus, burning, or irritation (worse with intercourse), erythema, edema, and excoriation • Thick, white (cottage cheese-like) vaginal discharge • Symptoms aggravate before menses
Diagnosis • pH is < 4.5 • Budding yeast, pseudohyphae (mycelia) on a wet mount (esp. the KOH preparation) • pH>4.5, large numbers of WBC: other infections? • Cultures are not routine • Other tests: urine tests, blood test
Treatment • Eliminate other causes, douche with alkaline solution • Medicated gels, creams, or suppositories applied directly to the vagina • Oral fluconazole (Diflucan), butoconazole (Femstat), clotrimazole (Gyne-lotrimin, Mycelex), miconazole (Monistat), and ticonazole (Vagistat) • Treatment of symptomatic sex partner
Complicated VVC Uncomplicated VVC Occurrence Clinical presentation Species of fungus Host status Response to therapy Infrequent Mild to medium Candida albican Immunocompetent Good Frequent recurrence Severe Other Candida sp. Immunoincompetent Poor
Intravaginal agents • Butoconazole 2% cream 5 g for 3 days,* • Clotrimazole 1% cream 5 g for 7-14 days,* • Clotrimazole 100 mg tablet for 7 days,* • Clotrimazole 100 mg tablet, two tablets for 3 days,* • Clotrimazole 500 mg tablet, one tablet in a single application,* • Miconazole 2% cream 5 g for 7 days,* • Miconazole 100 mg suppository, one suppository for 7 days,* • Miconazole 200 mg suppository, one suppository for 3 days,* • Nystatin 100,000-u vaginal tablet, one tablet for 14 days, • Tioconazole 6.5% ointment 5 g , single application,* • Terconazole 0.4% cream 5 g for 7 days,* • Terconazole 0.8% cream 5 g for 3 days,* • Terconazole 80 mg suppository, one suppository for 3 days.*
Trichomoniasis (Trich) • Accounts for 15-20% of vaginitis, 2-3 million /y in US • Infection with the single-celled parasite • Sexually transmitted disease • Occurs in both men and women: most men asymptomatic • Often associated with other STDs, assists AIDS spread • Microscopic examination or culturing evidence of presence of parasites in the vaginal discharge
Pathogenesis • Pear-shaped flagella, undulating membrane • Axis- spear-like protrusion, high motility • 2-3 times the size of a PMN leukocyte • High adaptability to environment • Favorable living environment: pH 5.2-6.6 • Compete for glycogen and thus reduce pH • Habitat: vagina, urethral, paraurethral gland, bladder, male genitalia
Clinical manefestitaion • Profuse, yellow-greenish, thin, frothy discharge with nasty odor • Purulent (mixed infection) • Itchy, pain burning, urinary irritation, asymptotic • Intensely inflamed vulva and vaginal wall, petechia (strawberry), frothy discharge in the posterior fornix
Diagnosis • Wet mount preparation: in normal saline • Culture • PCR
Treatment • Metronidazole 500 mg bid for 7 days or a single dose of 2 g po • 200 mg tablet or suppository • Treat of sex partner, avoid intercourse • Adverse effects: nausea, a metallic taste; severe nausea with vomiting is more common with the single dose • Metronidazole contraindicated during early pregnancy and lactation
Alternative treatment of vulvovaginal infections • Rebalance vaginal flora: L. acidophilus and L. bifidus, p.o. or vaginal application • Garlic, herbs • Acidify or alkaline the pH • Topical application of progesterone cream • Dietary modification and nutritional supplementation • Personal hygiene • Excessive douching should be avoided
Prognosis • Most women respond well to medications • Left untreated, can lead to: PID, endometritis, postsurgical infections, and spread AIDS virus • Cautious use of OTC yeast treatments • Use condoms to avoid STD
BV VVC Trich Pruritis mild or - Profuse discharge Severe pruritis burning Profuse discharge Mild pruritis Symptoms Features of discharge Vaginal mucosa Vaginal pH Whiff test Microscopic Thick, cheese-like or curdy Whitish, milky, fishy Frothy, thin, purulent Edematous, inflamed Edematous,inflamed, petechia Normal <4.5 >5 ( 5-6.5) >4.5 (4.7-5.7) negative positive negative Clue cells Minimum WBC Mycelial thread Spores Some WBC Trichomanos Lots of WBC
Cervicitis • Inflammatory process in cervical epithelium and stroma • Result in ascending infection • Acute or chronic • Acute cervicitis: caused by infections such as gonorrhea, chlamydia, or herpes, confused with vaginitis. • Chronic cervicitis: common in women following childbirth, pregnancy OC, unknown reasons • Less commonly, hypersensitivities to certain chemicals
Acute cervicitis • Caused by infections (gonorrhea, chlamydia, or herpes) • Accompanying vaginal and urinary irritability • Mucopurulent cervicitis (MPC): a yellow or green endocervical exudate visible in the endocervical canal or on an endocervical swab specimen • General erythema, ulcers, erosions, petechia • Diagnosis: discharge smear (30 PMN/ HPF) or culture, PCR, ELISA • Antibiotic agents
Chronic cervicits • Chronic cervicitis: common following childbirth. associated with pregnancy and OCP, hypersensitivities to chemicals (in spermicides, latex, and tampons), persistent bacterial invasion, inadequately treated acute cervicits • Main causative agent: staphylococci, rare causes (chlamydia trachomatis, tuberculosis)
Pathology • Cervical erosion • Absence of squamous epithelium from part of the ectocervical area • A raised red area • Granulation • Torn cervix with everted lips
Three types • Simple • Granular • Papilliform Degrees: I, II, III
Pathology • Cervical polyp • Nabothian cyst:retention cyst of cervical glands • Cervical hypertrophy • Endocervicitis