Download
1 / 1
10 likes | 134 Views
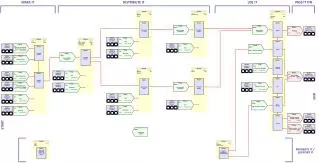
Under the hood Offsite servers Connection via Citrix servers Monitor data stream converted and forwarded by Capsule Technologies to MDIL to CPA Clinical data maintained in a cluster with one server and one on standby. SQL restore points every 15 minutes

E N D
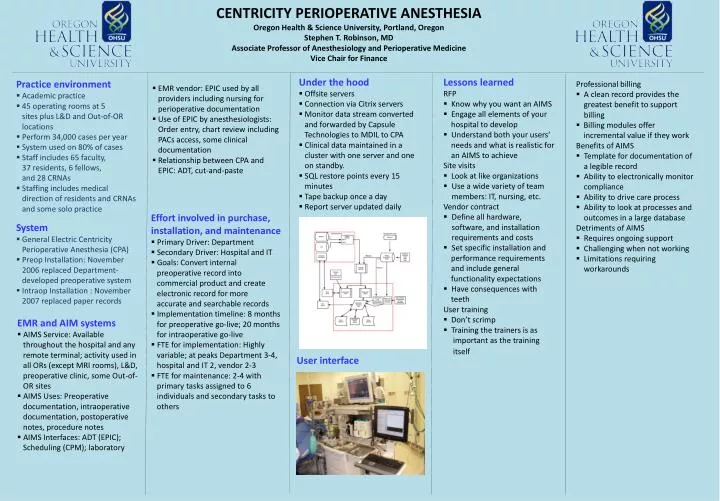
Under the hood • Offsite servers • Connection via Citrix servers • Monitor data stream converted • and forwarded by Capsule • Technologies to MDIL to CPA • Clinical data maintained in a • cluster with one server and one • on standby. • SQL restore points every 15 • minutes • Tape backup once a day • Report server updated daily • Lessons learned • RFP • Know why you want an AIMS • Engage all elements of your • hospital to develop • Understand both your users‘ • needs and what is realistic for • an AIMS to achieve • Site visits • Look at like organizations • Use a wide variety of team members: IT, nursing, etc. • Vendor contract • Define all hardware, software, and installation requirements and costs • Set specific installation and • performance requirements • and include general • functionality expectations • Have consequences with • teeth • User training • Don’t scrimp • Training the trainers is as • important as the training • itself • Practice environment • Academic practice • 45 operating rooms at 5 • sites plus L&D and Out-of-OR • locations • Perform 34,000 cases per year • System used on 80% of cases • Staff includes 65 faculty, • 37 residents, 6 fellows, • and 28 CRNAs • Staffing includes medical • direction of residents and CRNAs • and some solo practice • Professional billing • A clean record provides the • greatest benefit to support • billing • Billing modules offer incremental value if they work • Benefits of AIMS • Template for documentation of • a legible record • Ability to electronically monitor • compliance • Ability to drive care process • Ability to look at processes and • outcomes in a large database • Detriments of AIMS • Requires ongoing support • Challenging when not working • Limitations requiring • workarounds • EMR vendor: EPIC used by all • providers including nursing for • perioperative documentation • Use of EPIC by anesthesiologists: • Order entry, chart review including • PACs access, some clinical • documentation • Relationship between CPA and • EPIC: ADT, cut-and-paste CENTRICITY PERIOPERATIVE ANESTHESIA Oregon Health & Science University, Portland, OregonStephen T. Robinson, MDAssociate Professor of Anesthesiology and Perioperative MedicineVice Chair for Finance • System • General Electric Centricity • Perioperative Anesthesia (CPA) • Preop Installation: November • 2006 replaced Department- • developed preoperative system • Intraop Installation : November • 2007 replaced paper records • Effort involved in purchase, installation, and maintenance • Primary Driver: Department • Secondary Driver: Hospital and IT • Goals: Convert internal • preoperative record into • commercial product and create • electronic record for more • accurate and searchable records • Implementation timeline: 8 months • for preoperative go-live; 20 months • for intraoperative go-live • FTE for implementation: Highly • variable; at peaks Department 3-4, • hospital and IT 2, vendor 2-3 • FTE for maintenance: 2-4 with • primary tasks assigned to 6 • individuals and secondary tasks to • others • EMR and AIM systems • AIMS Service: Available • throughout the hospital and any • remote terminal; activity used in • all ORs (except MRI rooms), L&D, • preoperative clinic, some Out-of- • OR sites • AIMS Uses: Preoperative • documentation, intraoperative • documentation, postoperative • notes, procedure notes • AIMS Interfaces: ADT (EPIC); • Scheduling (CPM); laboratory • User interface