Download
1 / 39
390 likes | 612 Views
Musculoskeletal System. Temple College EMS Professions. Musculoskeletal System. Bones Muscles Cartilages Tendons Ligaments. Skeleton. Support against gravity Movement Protection Production of blood cells Storage of calcium, phosphorus. Cranium Frontal Parietal Temporal Occipital.

E N D
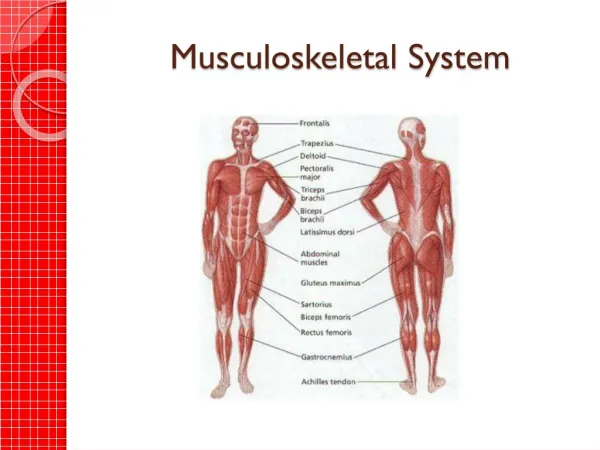
Musculoskeletal System Temple College EMS Professions
Musculoskeletal System • Bones • Muscles • Cartilages • Tendons • Ligaments
Skeleton • Support against gravity • Movement • Protection • Production of blood cells • Storage of calcium, phosphorus
Cranium Frontal Parietal Temporal Occipital Face Mandible Maxilla Zygoma Nasal bones Skull
Spinal Column • Cervical: 7 vertebrae • Thoracic: 12 vertebrae • Lumbar: 5 vertebrae • Sacrum: 5 vertebrae (fused) • Coccyx: 4 vertebrae (fused)
Thorax • 12 pairs of ribs • Sternum • Protects heart, lungs
Pelvis • Bony ring • Two innominate bones, each made of 3 fused bones • Ilium • Ischium • Pubis
Lower Extremity • Femur (largest bone in body) • Patella (knee cap) • Tibia (shin bone) • Fibula • Tarsals • Metatarsals • Phalanges
Upper Extremity • Shoulder girdle • Scapula • Clavicle • Humerus • Radius • Ulna • Carpals • Metacarpals • Phalanges
Muscles • Maintain posture, allow movement • 3 types: • Skeletal (Striated) • Smooth (Involuntary) • Cardiac
Skeletal Muscles • Voluntary muscles • Attach to bones by tendons that cross joints • Shortening of muscle moves joint
Smooth Muscles • Carry out involuntary movements • Located in walls of: • GI tract • GU tract • Respiratory tract • Blood vessels
Cardiac Muscle • Found only in heart • Automaticity • Can initiate own contractions without external stimulation
Joints • Joining points of bones • Bone-ends covered with cartilage • Ligaments connect bone-to-bone • Inner surface of joint capsule lined with synovial membrane • Produces synovial fluid • Lubricates joint
Extremity Trauma Temple College EMS Professions
Fracture • Break in bone’s continuity
Fracture Causes • Direct force • Indirect force • Twisting forces (torsion) • Diseases of bones (pathological fractures) • Osteoporosis • Tumors
Open vs. Closed Fractures • Closed = skin over fracture site intact • Open = break in skin over fracture site • Bone ends do not have to be exposed • Small opening in skin communicating with fracture site = open fx • Open fractures more serious due to external blood loss, possible infection
Fractures One of the most important things we do in EMS is prevent closed fractures from becoming open ones
Fracture Types • Transverse: fracture is at 90o angle to shaft • Oblique: fracture is at an angle other than 90o to shaft • Spiral: fracture coils through shaft of bone like a spring
Fracture Types • Impacted: bone ends driven into each other • Comminuted: bone broken into >3 pieces
Fracture Types • Greenstick • Shaft of bone not completely broken • Compressed on one side, splintered outward on other • What group of patients does this type of fracture occur in?
Fracture Signs • Deformity • Tenderness • Usually point tenderness • Overlies fracture site • Inability to use limb • Reliable sign of significant injury if present • Reverse is not true
Fracture Signs • Swelling, ecchymosis • Exposed fragments • Crepitus • Grating of bone ends • May be heard or felt • Do NOT actively seek
Dislocation • Displacement of bones from normal positions at joint
Dislocation Signs • Deformity • Swelling, ecchymosis about joint • Pain/tenderness in joint • Loss of motion usually perceived as “locked” joint
Sprains • Partial, temporary dislocations • Result in tearing of ligaments • Bone ends NOT displaced from normal positions
Sprain Signs • Tenderness • Swelling, ecchymosis • Inability to use extremity • No deformity
Sprains Degree of joint dislocation at time of injury cannot be determined during exam Extensive damage to neural or vascular structures may have occurred
Strains • “Muscle pull” • Injury to musculotendenous unit • Pain on active motion • Pain not present on passive motion
Assessment • Perform initial (primary) assessment • Locate, treat life-threats • Assess for injuries of head, chest, abdomen, pelvis • Assess distal neurovascular function
Assessment • With exception of pelvic, possibly femur fractures, orthopedic injuries are NOT life-threatening. • Do NOT let spectacular orthopedic injury distract you from ABCs • It’s the unobviousthings that kill patients!
Assessment • Evaluation must ALWAYS be done of distal neurovascular function. • Pulse • Skin color • Capillary refill • Sensation • Movement
Management • Splinting • Prevents further movement at injury site • Limits tissue damage, bleeding • Eases pain
Management • When in doubt • It is difficult to differentiate fractures, dislocations and sprains SPLINT
Principles of Splinting • DoNOT move patients before splinting unless patient is in danger • Remove clothes to allow inspection of limb • Note, record distal neurovascular function before, after splinting
Principles of Splinting • Cover wounds with dry, sterile compression dressings • Fractures: splint joint above, below fracture • Dislocations: splint bone above, below joint
Principles of Splinting • Minimize movement • Support injury until splinting completed • Pad splint to avoid local pressure
Principles of Splinting • Angulated fractures • Realign before splinting • If resistance, pain encountered stop, immobilize as is • Dislocations • Splint as is unless circulation compromised • Attempt to reposition once to restore pulse • If resistance, pain encountered stop, immobilize as is