Download
1 / 41
420 likes | 949 Views
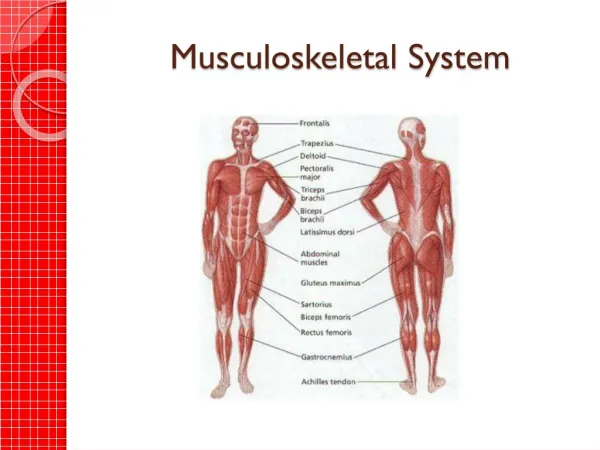
Musculoskeletal System. SPRAINS Occurs due to microfailure of collagen fibers secondary to stress exceeding their physiologic capacity. SEVERITY OF LIGAMENT INJURY FIRST-degree sprain: Minimal pain , no detectable joint instabiliy

E N D
SPRAINS • Occurs due to microfailure of collagen fibers secondary to stress exceeding their physiologic capacity
SEVERITY OF LIGAMENT INJURY • FIRST-degree sprain: Minimal pain , no detectable joint instabiliy • Treat symptomatically and return to full activity within a few days • Second –degree sprain :severe pain, minimal joint instability ,partial ligament rupture, 50% decrease in ligament strength and stiffness.
Treatment : • Rehabilitative exercise • Brace for support • Avoidance of physical activity
Third-degree sprain • Severe pain during course of injury • Joint completely unstable • Ligament can’t support any load • Treatment :surgery
FRACTURES • It is a break in the continuity of the bone • Close fracture :skin intact
Open fractures • Fracture communicate with the external environment due to a breach of the soft tissue • True orthopedic emergency • Prognosis dependent on extent of soft tissue injury and by type /level of bacterial contamination
Treatment plan • Prevent infection • Restore soft tissues • Achieve bone union • Early joint motion and muscle rehabilitation
Pathologic fracture • Occurs due to minimal trauma on a bone weakened by preexisting disease • Predisposing conditions :primary or metastatic carcinoma, cyst, enchodroma, giant cell tumors ,osteomalacia, osteogenesis imperfecta, scurvy , rickets, and Paget’s disease • Treatment : treat the broken bone , diagnose and treat the underlying condition
STRESS OR FATIGUE FRACTURE • Complete fx resulting from repetitive application of minor trauma • Most stress fx occur in Lower ext • Affect people involved in sports, military recruits • Xray can be normal • Pain occurs only with activity • Treatment : decrease physical activity
Comminuted fracture : • Bone is divided into more than 2 fragments • Greenstick fracture : • Incomplete and angulated of the long bone • Very common in children • Treatment: complete the fx and immobization
Fat embolism fracture: • Acute respiratory distress sd caused by realease of fat droplets from the marrow as may occur secondary a long bone fx • Signs&symtoms • Sx occur immediately or 2 to 3 days after trauma • SOB • Confusion, restlessness, disorientation, stupor or coma
Fleeting petechial rash on chest and conjunctiva • Fever,tachycardia • DIAGNOSIS : • ABG : PO2 < 60 mm Hg • CX-ray :progressive snowstorm-like infiltration • Presence of fat globules in urine is pathognomonic
Treatment • Administer O2 • Heparin • Prevent fat embolism sd by careful stabilization of fx
Typical scenario: A 25 y/o male complaints of difficulty breathing .His family notes he is acting a little confused , and that he has a spotty purplish rash. Two days ago , he sustained a femur fx after a high-speed motor vehicle collision.
Remember classic triad for fat embolism • Confusion • Dyspnea • petechiae
SHOULDER DISLOCATION: • Anterior dislocaton • High risk of recurrence 70 % • Occurs in younger than 30 y/o • Types : subcoracoid most common, subclavicular , subglenoid • Mechanism :abduction and external rotation of the arm causing strain on anterior capsule and glenohumeral ligaments
Signs&Symptoms: • Arms held to the side • Patients resists medial rotation and adduction • Prominent acromion • Loss of normal rounded shoulder contour
Posterior dislocation • Diagnosis missed in 60 % • Precipitated by convulsion,seizure, electrical shock • Types :subacromial, most common • Mechanism :internal rotation and adduction
Signs &Symptoms • Patient hold arm medially rotated and to the side • Abduction limited • External rotation limited • Flattening of anterior aspect of shoulder
Complications common to all dislocations • Palpate radial pulse to check axillary artery • Check sensory component of axillary nerve by assessing sensation over the lateral part of upper arm
Anterior dislocation complications: • Rotator cuff tear • Coracoid fractures • Greater tuberosity • Posterior dislocation: • Fractures of the lesser tuberosity
Treatment • Reduction and immobilization • Surgery if needed
COMPARTMENT SYNDROMES • Increased pressure within a limited space comprises the circulation and function of tissues within that closed space • Theories of tissue ischemia • Increased pressure leads to decreased transmural pressure,causing arterioles to close
Causes : • Fractures • Soft tissue crush injuries • Vascular injuries • Drug overdose with prolonged limb compression • Burn injuries • Trauma
Signs &Symptoms: 6P • Pain :deep, unremitting,and poorly localized.Pain increases with passive stretching of involved muscle • Pallor :not necessary for diagnosis • Paresthesias :of cutaneous distribution supplied by the compressed nerve is an early sign • Paralysis :occurs after ischemia is well established • Pulselessness :shown to occur late at times
Diagnosis • Measure pressure within compartment • Pressure < 30 mm Hg will not produce a compartment syndrome • Pressure >30mm Hg is an indication for fasciotomy • Treatment : • Complete fasciotomy
0steomyelitis • Epidemiology :mainly affects children • Pathophysiology • 1- bacteria lodge in end artery of metaphysis and multiply • 2-local increase in serum and white blood cells • 3-decrease in blood flow and pressure necrosis • 4- pus moves to haversian and medullary canals • 5-goes beneath the periosteum
Signs&symptoms • Hx infection or trauma • Significant pain in the affected area,anorexia, fever,nausea • Limited joint motion, tenderness and swelling of soft tissue
Diagnosis • Elevated wbc,erythrocyte sedimentation • Deep circumferential, soft-tissue swelling
Treatment • Medical :iv antibiotic • Surgery
Low back pain • Epidemiology • 4 out 5 people suffer from low back pain • Incidence 15 -20 %, male >females • Often back pain is a sx of systemic illness such as primary or metastatic neoplasm , infection disease or inflammatory disorder
History • Localization of the pain • Character of pain • Hx of pain development and how it affects everyday of pain • Hx of weight loss, malaise, fever,Gu
Physical examination • 1- straight leg-raising test:positive in nerve root irritation • 2-check for reflexes and motor and sensory deficits • 3-check spine for range of motion • 4- bowel and bladder sx are suggestive of cauda equina syndrome
Diagnosis • 1- xray of lumbar spine • 2-MRI if xray negative • 3-technetium bone scan and gallium scan can be done if an infection of the spine is suspected
Treatment • 1- Rule out a serious pathologic condition • 2- goal is early return to normal activities • 3-NSAIDs • 4- physical and occupational therapy programs