Download
1 / 29
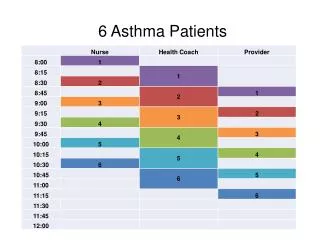
380 likes | 1.1k Views
Perioperative Assessment of Asthma Patients. Presented by Ri 胡殿詮 冉景儀 Instructed by CR 劉治民 Date: 2006/03/28. Introduction: Peri-OP Assessment of Asthma Patients. PPC (postoperative pulmonary complications) of asthma Atelectasis Pneumonia or bronchitis

E N D
Perioperative Assessment of Asthma Patients Presented by Ri 胡殿詮 冉景儀 Instructed by CR 劉治民 Date: 2006/03/28
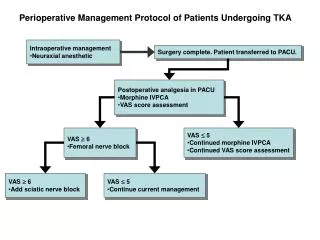
Introduction: Peri-OP Assessment of Asthma Patients • PPC (postoperative pulmonary complications) of asthma Atelectasis Pneumonia or bronchitis Bronchospasm (reflex bronchoconstriction during airway instrumentation) Hypoxemia Respiratory failure Prolonged mechanical ventilation Intrapulmonary shunting Pneumothorax Retained secretions • Difficulty in PPC research & epidemiologic study Lack of consensus in PPC definition
Objects • Correlation between anesthesia & PPC • Correlation between surgery & PPC • Preoperative assessment of asthmatic patients • Suggestion for surgical asthmatic patients
Correlation Between Anesthesia & PPC: GA • Reflex bronchoconstriction during airway instrumentation ASA: severe bronchospasm → 90% death or irreversible brain damage • Mechanical & functional changes of pulmonary system during GA Alteration in diaphragm movement (more ventilation in upper lung & less ventilation in lower lungs) → V/Q mismatch → Shunt & dead-space ventilation, increased AaO2 gradient → Reduction in FRC → Atelectatic plaques in dependent portion of lungs • Airway hyper-responsitivity during GA ↓Number & activity of alveolar macrophages ↓Mucociliary clearance ↓Surfactant release ↑Alveolar-capillary permeability ↑Activity of pulmonary NOS ↑Sensitivity of pulmonary vasculature to neorohumoral mediators
Correlation Between Anesthesia & PPC: GA • Neuro-muscular blockers ↓ Hypoxic drive to ventilate More common in Pancuronium use • Neuro-chemical changes during GA ↓ Peripheral chemoreceptor response to hypoxemia ↓ CNS response to hypercapnia (both IV & inhaled agent at subanesthetic concentration as 0.1 MAC) Prolonged postoperative hypoxemia GA → Increased PPC rate!
Correlation Between Anesthesia & PPC Strategy • Regional anesthesia No requirement of airway manipulation Less impact on ventilatory control No ”unopposed parasympathetic hyperactivity” No neuromuscular blockade • Post-OP epidural analgesia However…. • No evidence of lower PPC rate in regional anesthesia or post-OP epidural analgesia • Warner’s study of > 1500 asthma patients: PPC rates for regional & regional anesthesia were similar Warner DO et al., Perioperative respiratory complications in patients with asthma. Anesthesiology 85 (1996), pp. 460–7
Correlation Between Anesthesia & PPC: GA • Bronchospasm prevention: Pretreatment with lidocaine & salbutamol → significantly attenuate FEV1 decrease Salbutamol → Lidocaine Salbutamol → Dyclonine Saline → Lidocaine Saline → Dyclonine H. Groeben, M. Schlicht, S. Stieglitz et al., Both local anesthetics and albutamol pretreatment affect reflex bronchoconstriction in volunteers with asthma undergoing awake fiberoptic intubation. Anesthesiology97 (2002), pp. 1445–1450
Correlation Between Surgery & PPC Risk group: thoracic and upper abdominal surgery • Diaphragm dysfunction (due to reflex inhibition of phrenic nerve output) → Decreased vital capacity & FRC (~50% of baseline after laparotomy, returning toward normal over 1-2 weeks) → V/Q mismatch → Atelectasis, hypoxemia, etc. • Surgical trauma → Increased airway tone & reactivity → Exposure of airway irritants → bronchospasm!
Correlation Between Surgery & PPC Strategy • Laparoscopic procedures: better or not? Improved FEV1, FRC, arterial oxygenation, ventilation However…. • Still associated with diaphragm dysfunction • No evidence of PPC rate reduction
Preoperative Assessment of Asthmatic Patients • History taking & Identification of risk group • Pulmonary function test • ABG or other laboratory study
Preoperative Assessment of Asthmatic Patients: Risk Risk group for PPC • General Age > 70y/o Cigarette smoking Renal failure Poor nutrition • Asthma related Recent asthma attack Recent use of anti-asthma therapy for symptomatic control Past history of endotracheal intubation for asthma management • Surgery & anesthesia related Emergent surgery Thoracic, vascular, or upper abdominal surgery Blood loss > 4U PRBC (2000mL) Anesthetic time > 180 minutes General anesthesia with endotracheal intubation
Preoperative physical status of patients according to the American Society of Anesthesiologists
Preoperative Assessment of Asthmatic Patients: Risk Kroenke et al.: ASA classification of asthma patients vs. PPC • Class 4: ~46% • Class 3: ~28% • Class 2: ~10%
Preoperative Assessment of Asthmatic Patients • History taking & Identification of risk group • Pulmonary function test • ABG or other laboratory study
Preoperative Assessment of Asthmatic Patients: PFT Pulmonary function test: Controversial! • Significance of Pre-OP PFT: Identification of asymptomatic patients with chronic lung disease, rather than risk stratification of clinically-diagnosed asthmatic patients • Application in Pre-OP assessment Assess bronchospasm induced by provocation test Response to bronchodilators
Preoperative Assessment of Asthmatic Patients: PFT • H.R. Smith et al.(1992) FEV1 < 80% of predicted values or airway resistance > 0.35kpascal/l/s → Repeat test 15-20 minutes after beta-2 agonist inhalation → If improvement >15% → Pre-OP beta-2 agonist • GINA Workshop Report (updated 2004) If FEV1 < 80% of personal best → brief course of steroid Dose: prednisolone 40~60 mg/day Start time: 1-2 days prior to surgery End time: within 24 hours after surgery • H.R. Smith, C.G. Irvin and R.M. Cherniack, The utility of spirometry in the diagnosis of reversible airway obstruction. Chest101 (1992), pp. 1577–1581 • GINA Workship Report (updated 2004). Global Strategy for the Asthma Management and Prevention.
Preoperative Assessment of Asthmatic Patients • History taking & Identification of risk group • Pulmonary function test • ABG or other laboratory study
Preoperative Assessment of Asthmatic Patients: ABG • Baseline ABG: not necessary No help in risk assessment or stratification • Other laboratory test: no evidence of any improvement in pre-OP assessment for PPC • Pulse oximetry: non-invasive, cost-effective, supplements the history & PE findings
Suggestion: Pre-OP Assessment & Preparation History taking & risk identification • Age > 70y/o • Cigarette smoking • Renal failure • Poor nutrition • Use of systemic steroid within the past 6 months • Asthma severity • Recent Asthma attack • Past history of endotracheal intubation for asthma management • Emergent surgery • Thoracic, vascular, or upper abdominal surgery • Blood loss > 4U PRBC (2000mL) • Anesthetic time > 180 minutes • General anesthesia with endotracheal intubation • PFT: FEV1 < 80% of personal best
Suggested Protocol: Pre-OP Assessment & Preparation • Use of systemic steroid within the past 6 months → Regimen: Hydrocortisone 100mg q8h iv Start time: 1-2 days prior to surgery End time: within 24 hours after surgery • PFT: FEV1 < 80% of personal best → Regimen: Prednisolone 40-60 mg/day po Start time: 1-2 days prior to surgery End time: within 24 hours after surgery • No need of tapering dose • Prolong post-OP steroid use: increased infection rate, poor wound healing GINA Workship Report (updated 2004). Global Strategy for the Asthma Management and Prevention.
Suggested Protocol: Pre-OP Assessment & Preparation • Wheezing before OP Inhaled beta-2 adrenergic agents & corticosteroid → If no improvement, defer the elective surgery • Reversible airway obstruction or severe bronchial hyperreactivity Regimen: Methylprednisolone 0.5-1.0 mg/kg po & Salbutamol 3x2 puffs Start time: 48 hours prior to surgery M.T. Silvanus, H. Groeben and J. Peters, Corticosteroids and inhaled salbutamol in patients with reversible airway obstruction markedly decrease the incidence of bronchospasm after tracheal intubation. Anesthesiology 100 (2004), pp. 1052–1057. International Asthma Report, National Institute of Health, International consensus report on diagnosis and treatment of asthma. European Respiratory Journal 5 (1992), pp. 601–641
Suggested Protocol: Pre-OP Assessment & Preparation • Pretreatment of combined inhaled beta-2 agonist & systemic corticosteroid M.T. Silvanus, H. Groeben and J. Peters, Corticosteroids and inhaled salbutamol in patients with reversible airway obstruction markedly decrease the incidence of bronchospasm after tracheal intubation. Anesthesiology 100 (2004), pp. 1052–1057.
Suggested Protocol: Post-OP Care & Management • Serial ABG & CxR follow up • Peri-OP oxygen supplementation • Incentive spirometry • Adequate pain relief (avoid NSAID in patients with past history of aspirin-induced asthma) • Consider theophylline administration (bronchodilator, respiratory stimulant, diaphragm inotrope) • Consider post-OP epidural analgesia
Reference • Rock P, Passannante A. Preoperative assessment: pulmonary. Anesthesiology Clinics of North America 2004; 22:77-91. • GINA Workship Report (updated 2004).Global Strategy for the Asthma Management and Prevention. • Paul C. Tamul, William T. Peruzzi. Assessment and management of patients with pulmonary disease. Critical Care Medicine 2004; 32(4): S137-45. • H. Groeben. Strategies in the patient with compromised respiratory function. Best Practice & Research Clinical Anaesthesiology 2004; 18(4): 579-594 . • H. Groeben, M. Schlicht, S. Stieglitz et al., Both local anesthetics and albutamol pretreatment affect reflex bronchoconstriction in volunteers with asthma undergoing awake fiberoptic intubation. Anesthesiology 97 (2002), pp. 1445–1450 • Warner DO et al., Perioperative respiratory complications in patients with asthma. Anesthesiology 85 (1996), pp. 460–7 • H.R. Smith, C.G. Irvin and R.M. Cherniack, The utility of spirometry in the diagnosis of reversible airway obstruction. Chest 101 (1992), pp. 1577–1581 • M.T. Silvanus, H. Groeben and J. Peters, Corticosteroids and inhaled salbutamol in patients with reversible airway obstruction markedly decrease the incidence of bronchospasm after tracheal intubation. Anesthesiology 100 (2004), pp. 1052–1057. • International Asthma Report, National Institute of Health, International consensus report on diagnosis and treatment of asthma. European Respiratory Journal 5 (1992), pp. 601–641