Download
1 / 1
10 likes | 187 Views
Diffuse Melanosis in a Patient with Metastatic Melanoma. 1 Everett J, 2 Cardin MJ , 3 Solymoss S, 2 Jung S, 2 Fraser R, 1 Green L . 1 Department of Medicine, McGill University Health Center, Montreal, QC 2 Department of Pathology, McGill University Health Center, Montreal, QC

E N D
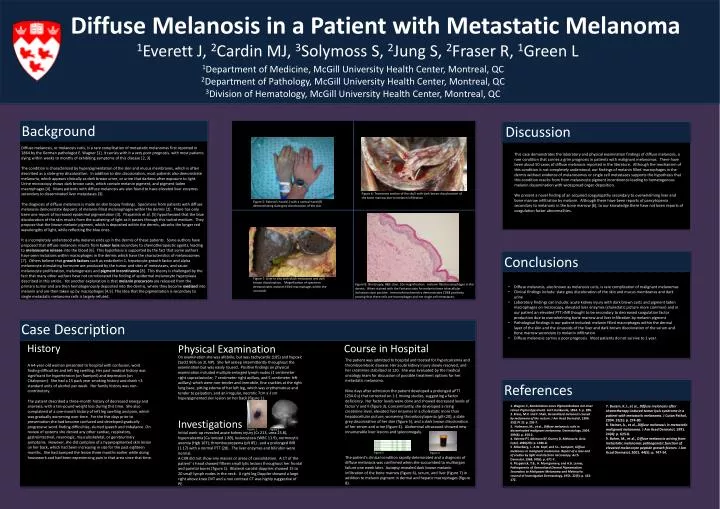
Diffuse Melanosis in a Patient with Metastatic Melanoma 1Everett J, 2Cardin MJ, 3Solymoss S, 2Jung S, 2Fraser R, 1Green L 1Department of Medicine, McGill University Health Center, Montreal, QC 2Department of Pathology, McGill University Health Center, Montreal, QC 3Division of Hematology, McGill University Health Center, Montreal, QC Background Discussion Diffuse melanosis, or melanosis cutis, is a rare complication of metastatic melanomas first reported in 1864 by the German pathologist E. Wagner [1]. It carries with it a very poor prognosis, with most patients dying within weeks to months of exhibiting symptoms of this disease [2, 3] The condition is characterized by hyperpigmentation of the skin and mucus membranes, which is often described as a slate-grey discoloration. In addition to skin discoloration, most patients also demonstrate melanuria, which appears clinically as dark brown urine, or urine that darkens after exposure to light. Urine microscopy shows dark brown casts, which contain melanin pigment, and pigment-laden macrophages [4]. Many patients with diffuse melanosis are also found to have elevated liver enzymes secondary to disseminated liver metastases [3]. The diagnosis of diffuse melanosis is made on skin biopsy findings. Specimens from patients with diffuse melanosis demonstrate deposits of melanin-filled melanophages within the dermis [2]. There has only been one report of increased epidermal pigmentation [3]. Fitzpatrick et al. [5] hypothesized that the blue discoloration of the skin results from the scattering of light as it passes through this turbid medium. They propose that the brown melanin pigment, which is deposited within the dermis, absorbs the longer red wavelengths of light, while reflecting the blue ones. It is incompletely understood why melanin ends up in the dermis of these patients. Some authors have proposed that diffuse melanosis results from tumor lysis secondary to chemotherapeutic agents, leading to melanosome release into the blood [6]. This hypothesis is supported by the fact that some authors have seen inclusions within macrophages in the dermis which have the characteristics of melanosomes[7]. Others believe that growth factors such as endothelin-1, hepatocyte growth factor and alpha melanocyte stimulating hormone are produced by the tumor and sites of metastases, and cause melanocyte proliferation, melanogenesis and pigment incontinence[8]. This theory is challenged by the fact that many other authors have not corroborated the finding of epidermal melanocyte hyperplasia described in this article. Yet another explanation is that melanin precursors are released from the primary tumor and are then hematogenously deposited into the dermis, where they become oxidized into melanin and are then taken up by macrophages [4,5]. The idea that the pigmentation is secondary to single metastatic melanoma cells is largely refuted. This case demonstrates the laboratory and physical examination findings of diffuse melanosis, a rare condition that carries a grim prognosis in patients with malignant melanomas. There have been about 50 cases of diffuse melanosis reported in the literature. Although the mechanism of this condition is not completely understood, our findings of melanin filled macrophages in the dermis without evidence of melanosomes or single cell metastases supports the hypothesis that this condition results from from melanocyte pigment incontinence leading to hematogenous melanin dissemination with widespread organ deposition. We present a novel finding of an acquired coagulopathy secondary to overwhelming liver and bone marrow infiltration by melanin. Although there have been reports of pancytopenia secondary to melanosis in the bone marrow [6], to our knowledge there have not been reports of coagulation factor abnormalities. Figure 6: Transverse section of the skull with dark brown discoloration of the bone marrow due to melanin infiltration Figure 5: Patient’s hand (L) with a normal hand (R) demonstrating slate grey discoloration of the skin Conclusions Figure 7: Liver in situ with black metastasis and dark brown discoloration. Magnification of specimen demonstrates melanin-filled macrophages within the sinusoids Figure 8: Skin biopsy, H&E stain, 10x magnification: melanin filled macrophages in the dermis. When stained with the Fontana stain for melanin these intracellular inclusions stain positive. Immunohistochemistry demonstrates CD68 positivity, proving that these cells are macrophages and not single cell metastases. • Diffuse melanosis, also known as melanosis cutis, is rare complication of malignant melanomas • Clinical findings include: slate grey discoloration of the skin and mucus membranes and dark urine • Laboratory findings can include: acute kidney injury with dark brown casts and pigment laden macrophages on microscopy, elevated liver enzymes (cholestatic picture more common) and in our patient an elevated PTT>INR thought to be secondary to decreased coagulation factor production due to overwhelming bone marrow and liver infiltration by melanin pigment • Pathological findings in our patient included: melanin filled macrophages within the dermal layer of the skin and the sinusoids of the liver and dark brown discoloration of the serum and bone marrow secondary to melanin infiltration • Diffuse melanosis carries a poor prognosis. Most patients do not survive to 1 year. Case Description History Course in Hospital Physical Examination On examination she was afebrile, but was tachycardic (105) and hypoxic (SaO2 96% on 2L NP). She fell asleep intermittently throughout the examination but was easily roused. Positive findings on physical examination included multiple enlarged lymph nodes (1 centimeter right supraclavicular, 7 centimeter right axillary, and 5 centimeter left axillary) which were non-tender and immobile, fine crackles at the right lung base, pitting edema of her left leg, which was erythematous and tender to palpation, and an irregular, necrotic 7cm x 3 cm hyperpigmented skin lesion on her back (figure 1). The patient was admitted to hospital and treated for hypercalcemia and thromboembolic disease. Her acute kidney injury slowly resolved, and her creatinine stabilized at 120. She was evaluated by the medical oncology team for discussion of possible treatment options for her metastatic melanoma. Nine days after admission the patient developed a prolonged aPTT (234.0 s) that corrected on 1:1 mixing studies, suggesting a factor deficiency. Her factor levels were done and showed decreased levels of factor V and II (figure 3). Concomitantly, she developed a rising creatinine level, elevated liver enzymes in a cholestatic more than hepatocellular picture, worsening thrombocytopenia (plt<20), a slate grey discoloration of her skin (figure 5), and a dark brown discoloration of her serum and urine (figure 4). Abdominal ultrasound showed new innumerable liver lesions and splenomegaly. The patient’s clinical condition rapidly deteriorated and a diagnosis of diffuse melanosis was confirmed when she succumbed to multiorgan failure one week later. Autopsy revealed dark brown melanin infiltration of the bone marrow (figure 6), serum, and liver (figure 7) in addition to melanin pigment in dermal and hepatic macrophages (figure 8). A 64-year-old woman presented to hospital with confusion, word finding difficulties and left leg swelling. Her past medical history was significant for hypertension (on Ramipril) and depression (on Citalopram). She had a 15 pack year smoking history and drank <3 standard units of alcohol per week. Her family history was non-contributory. The patient described a three-month history of decreased energy and anorexia, with a ten-pound weight loss during this time. She also complained of a one-month history of left leg swelling and pain, which was gradually worsening over time. For the five days prior to presentation she had become confused and developed gradually progressive word-finding difficulties, slurred speech and imbalance. On review of systems she denied any other cardiac, respiratory, gastrointestinal, neurologic, musculoskeletal, or genitourinary symptoms. However, she did complain of a hyperpigmented skin lesion on her back, which had been increasing in size for the past eighteen months. She had bumped the lesion three months earlier while doing housework and had been experiencing pain in that area since that time. References 1. Wagner, E, KombinationeinesPigmentkrebsesmiteinerreinenPigmentgeschulst. Arch Heilkunde, 1864. 5: p. 280. 2 .Klaus, M.V. and F. Shah, Generalized melanosis caused by melanoma of the rectum. J Am AcadDermatol, 1996. 35(2 Pt 2): p. 295-7. 3. Hofmann, M., et al., Diffuse melanosis cutis in disseminated malignant melanoma. Dermatology, 2004. 209(4): p. 350-2. 4. Valente PT, Atkinson BF, Guerry D, Melanuria.ActaCytol, 1985(29): p. 1026-8. 5 .Silberberg, I., A.W. Kopf, and S.L. Gumport, Diffuse melanosis in malignant melanoma. Report of a case and of studies by light and electron microscopy. Arch Dermatol, 1968. 97(6): p. 671-7. 6. Fitzpatrick, T.B., H. Montgomery, and A.B. Lerner, Pathogenesis of Generalized Dermal Pigmentation Secondary to Malignant Melanoma and Melanuria. Journal of Investigative Dermatology, 1954. 22(3): p. 163-172. 7. Busam, K.J., et al., Diffuse melanosis after chemotherapy-induced tumor lysis syndrome in a patient with metastatic melanoma. J CutanPathol, 2004. 31(3): p. 274-80. 8. Steiner, A., et al., Diffuse melanosis in metastatic malignant melanoma. J Am AcadDermatol, 1991. 24(4): p. 625-8. 9. Bohm, M., et al., Diffuse melanosis arising from metastatic melanoma: pathogenetic function of elevated melanocyte peptide growth factors. J Am AcadDermatol, 2001. 44(5): p. 747-54. Investigations Figure 1 Figure 2 Initial work-up revealed acute kidney injury (Cr 213, urea 25.8), hypercalcemia (Ca Ionized 1.89), leukocytosis (WBC 11.9), normocytic anemia (Hgb 107), thrombocytopenia (plt 85) , and a prolonged INR (1.17) with a normal PTT (28). The liver enzymes and bilirubin were normal. A CXR did not show any masses or areas of consolidation. A CT of the patient’ s head showed fifteen small lytic lesions throughout her frontal and parietal bones (figure 2). Bilateral carotid dopplers showed 15 to 20 small lymph nodes in the neck. A right leg Doppler showed a large right above knee DVT and a non contrast CT was highly suggestive of PE. Figure 3 Figure 4